
Andrew Dyson, Digital Health Business Consultant



We are excited to announce the recent changes and updates we have released into the Medirecords product. Below you will find a summary of each of the changes we have made.
The file size limit has been increased across MediRecords, to allow you to upload larger file sizes. This change affects the following areas within MediRecords:
You may now view the provider number for a contact from within the Health Professionals grid within Resources.

New mail merge fields have been added to the letter editor, so you may now import a patient’s Interested Parties and Usual GP directly from the patient’s record. These fields are found within the Patient table when editing a template or letter. When using these fields, the following will occur:
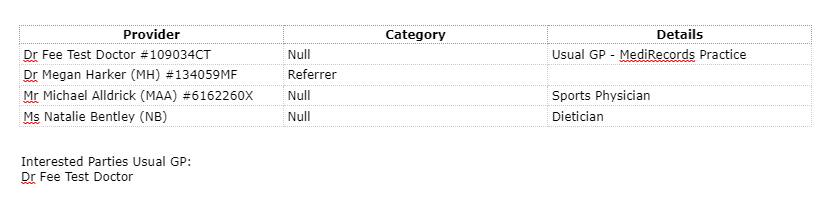
You may now search by a provider by entering their provider number into the search bar available at the top of the Health Professionals grid. Results will be returned when you have entered a minimum of 3 characters from the beginning of the provider number.
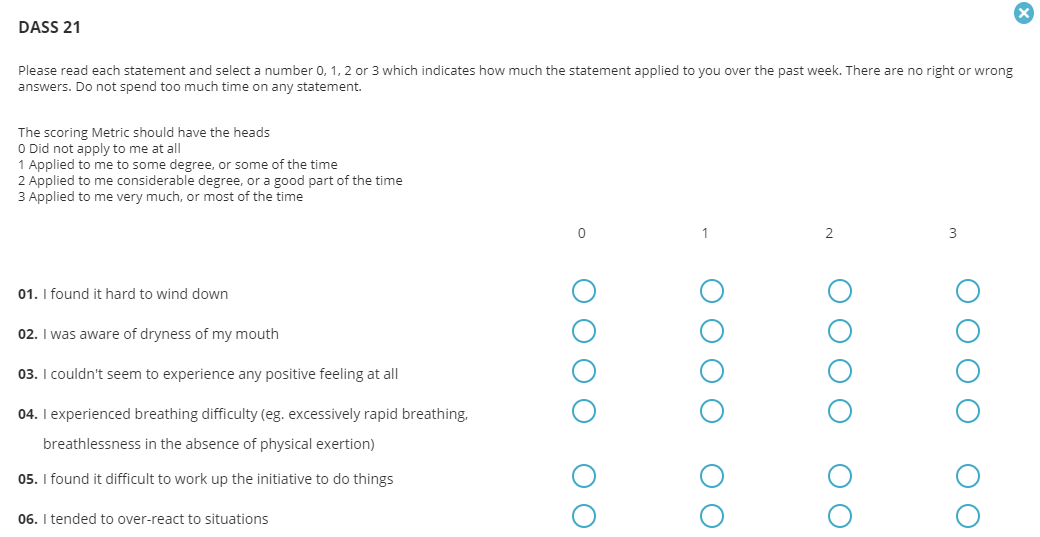
The DASS21 form is now available as an EPC template within the consultation window. Answering the questions will provide a scoring for each category, and an overall scoring with appropriate diagnosis.
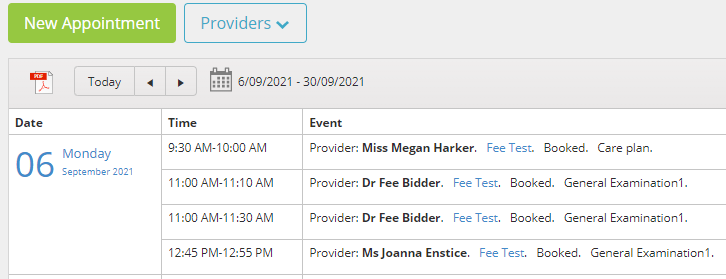
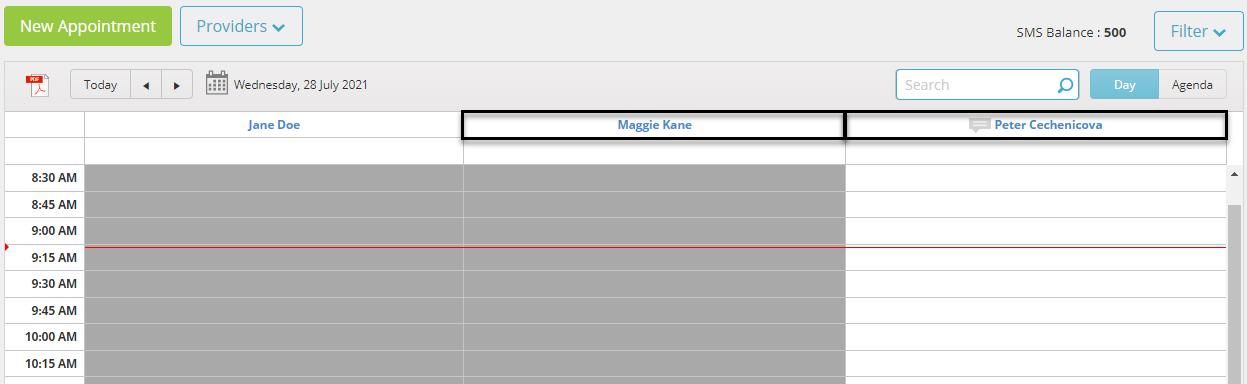
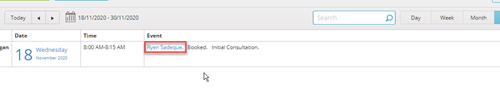
The Agenda view in Appointments will now display all appointments in chronological order, rather than grouping the appointments by provider. This improvement aims to improve the Agenda’s usefulness when looking to see the appointments booked for a certain patient, or provider.
When searching in the Health Professionals or Service Provider grids, you will no longer lose your search term after opening and closing a record. This assists with finding the correct contact record where a contact may have multiple records for different locations.
When applying filters within the Tasks/Activities window, you will now be able to apply separate filters for each patient.
These changes have come about from customers like you, who have given us their feedback. MediRecords is committed to continuous improvement to allow for ease of use of our product, so if you have any feedback, please let your account manager know!
See you next month for more exciting new features and functions within MediRecords.

We are excited to announce the recent changes and updates we have released into the Medirecords product. Below you will find a summary of each of the changes we have made.
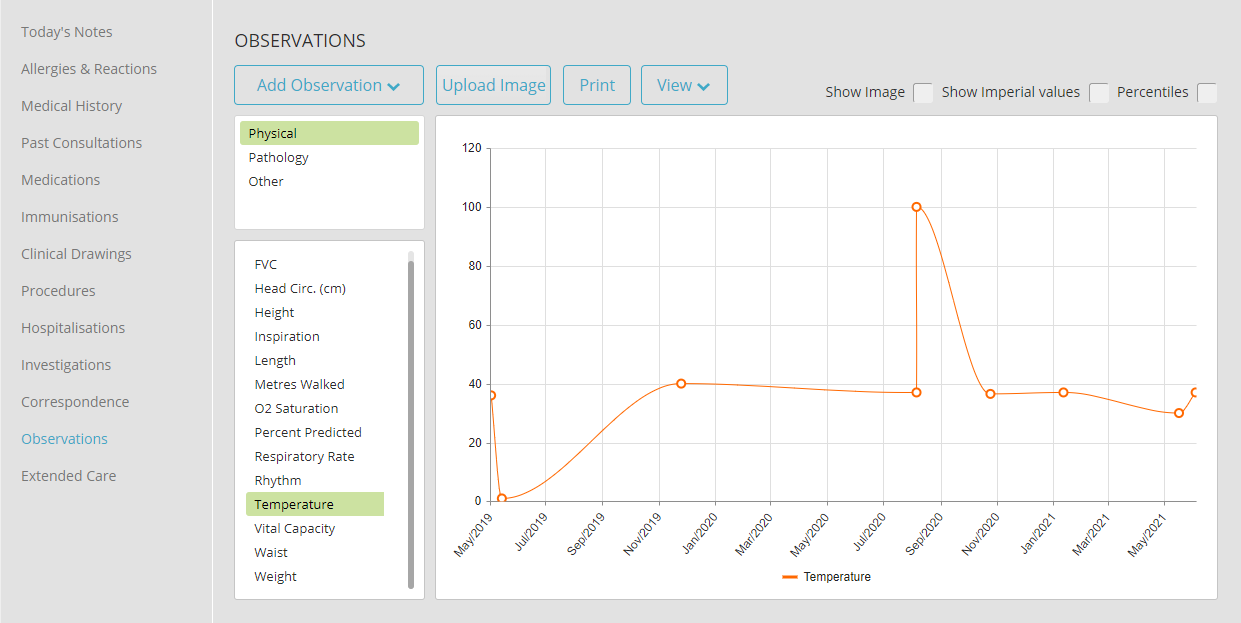
Improvements have been made to the Observations function, so that all observations may now appear within the timeline graph view, rather than a selected amount, improving visibility of a patient’s health over time.
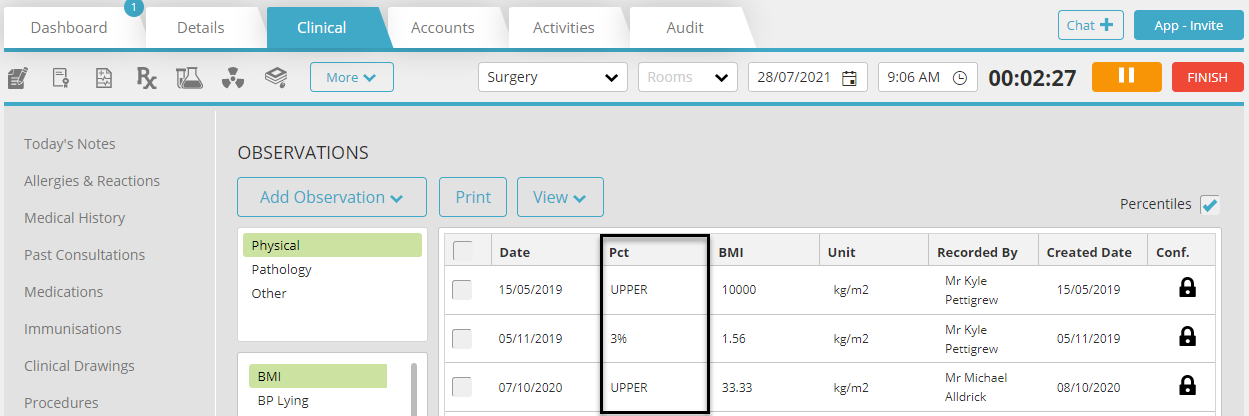
The PCT value will now display within the Observations grid when the Percentile tick-box has been selected.
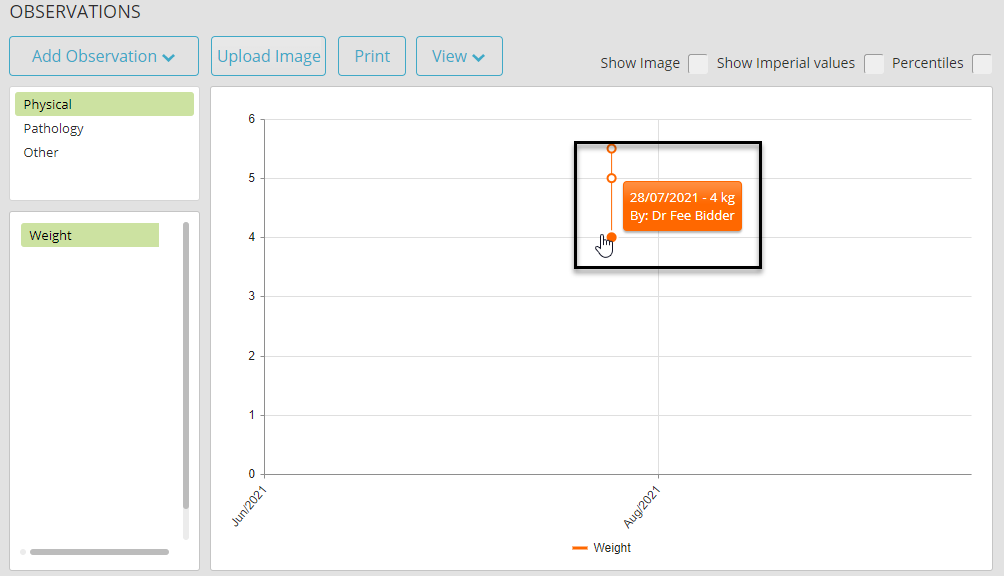
Hovering over an entry in the Observation Timeline view will now display the percentile value, the user who created the entry, and the date of entry.
Provider usernames have been updated within the Appointment Book to display First and Surname. If a status has been added to the provider and their full name exceeds the character limit, then only the provider’s surname will be displayed alongside the status.
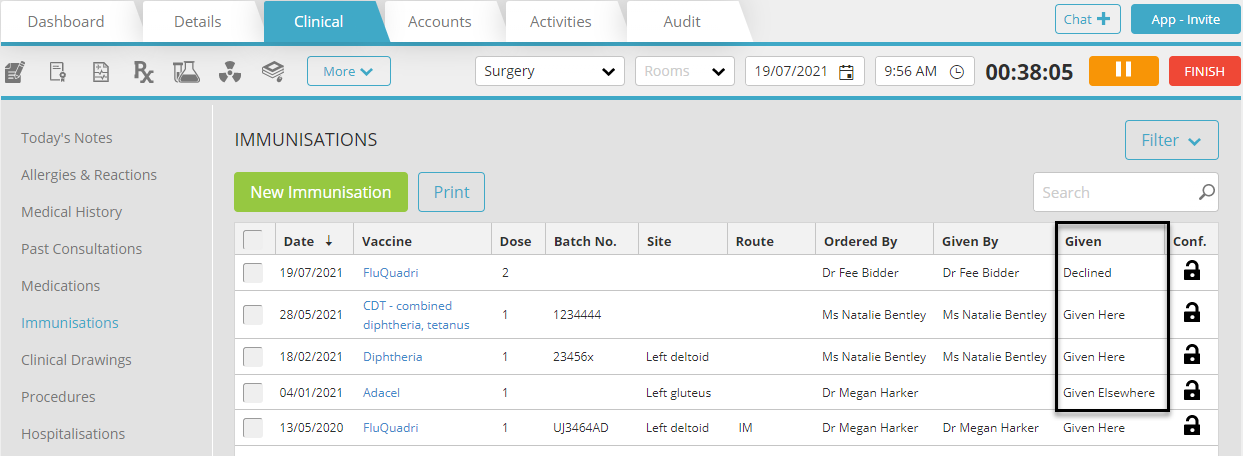
The Given Field is now available within the Immunisation Grid, so you may tell at a quick glance whether an immunization was given elsewhere, given within the clinic, or if the immunization was declined.
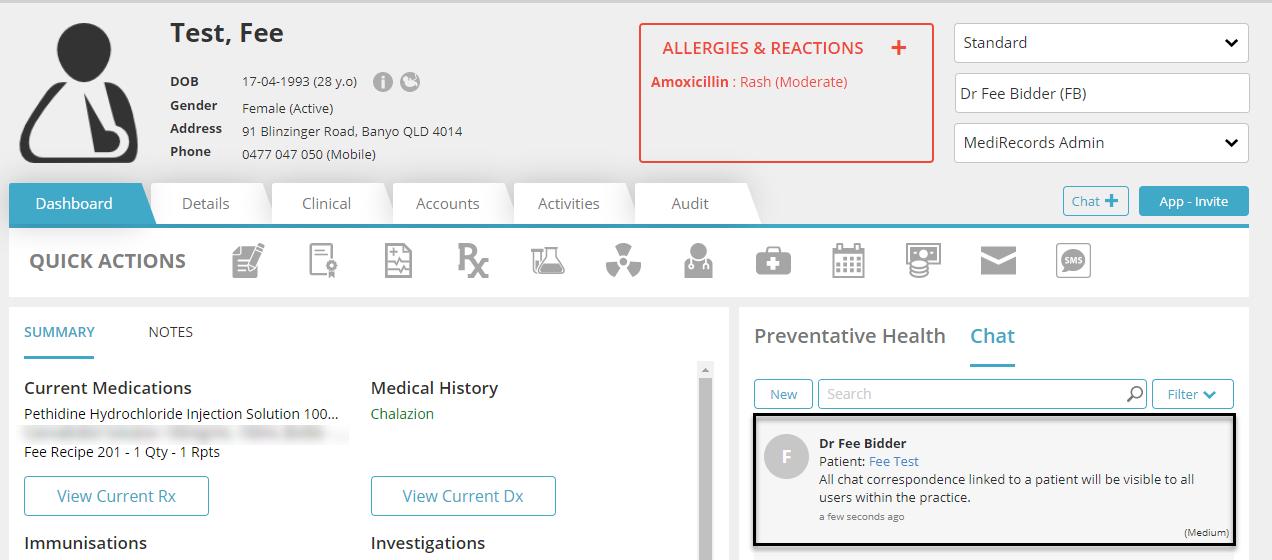
Users may now view all chat threads on a Patient Record Dashboard, regardless of who created the chat message or received it. This ensures that all chat correspondence is available on the Patient Record for all users.
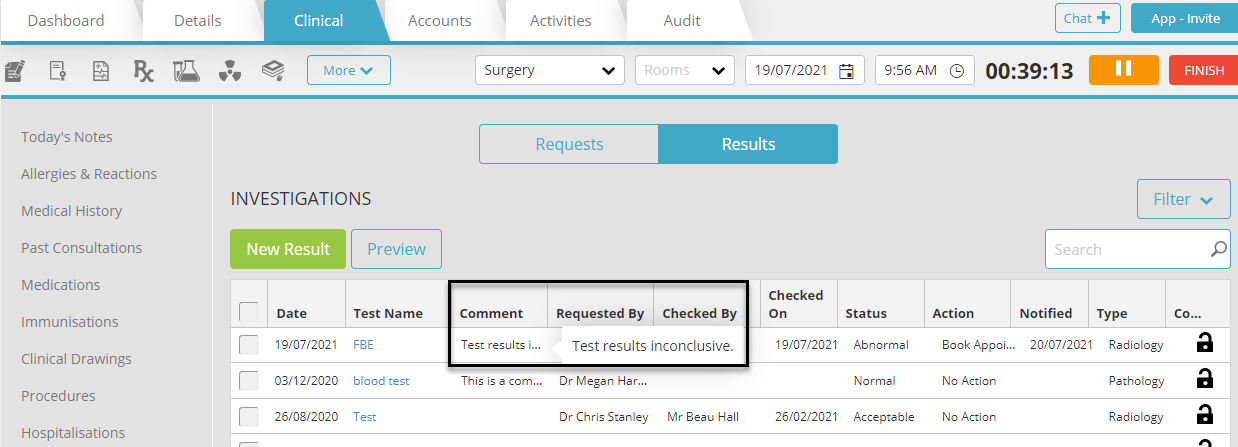
Now when viewing the Investigations grid, you may see any Comments that have been added to a result item. A preview of the comments will be displayed where space allows, and hovering over the preview will show the entire comment.
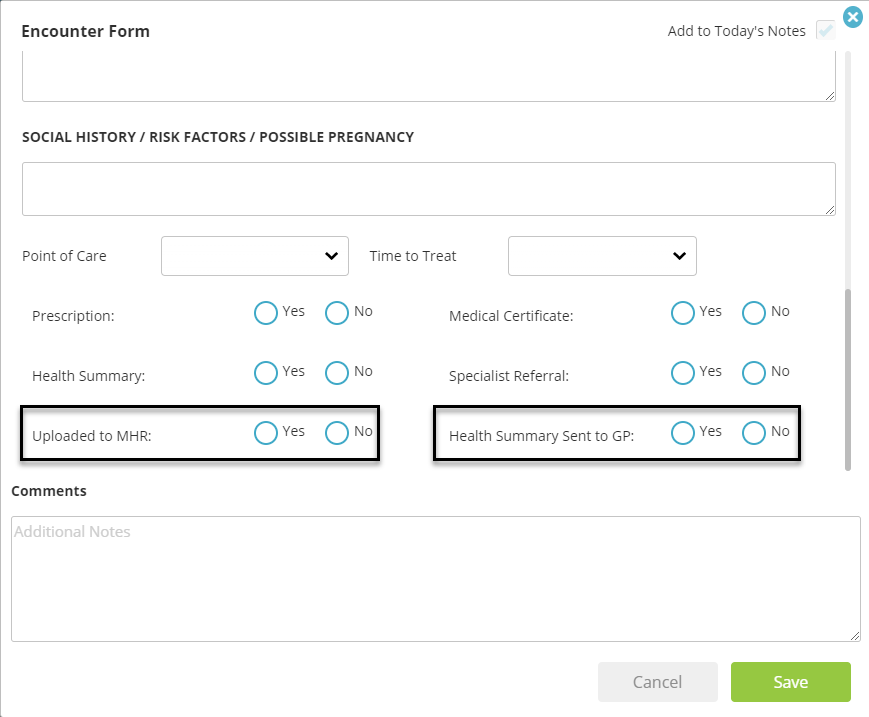
Checkboxes have been added to the Encounter Form, for “Uploaded to My Health Record”, and “Health Summary Sent to GP”, for practices using My Health Record functionality.
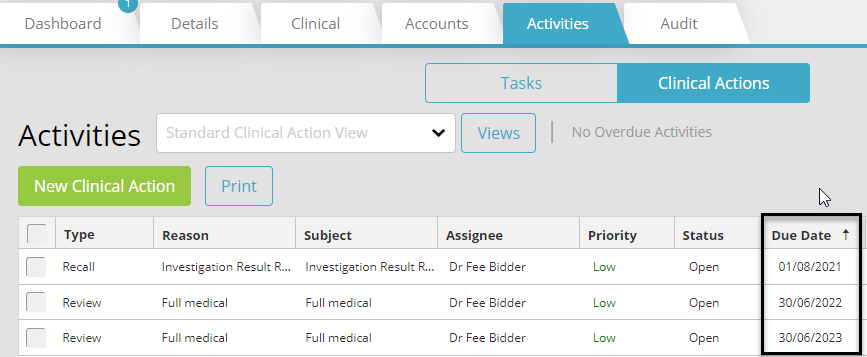
Activities will now be ordered by earliest due date first in both the patient record and within the Activities/Tasks window, to improve the prioritisation of Activities.
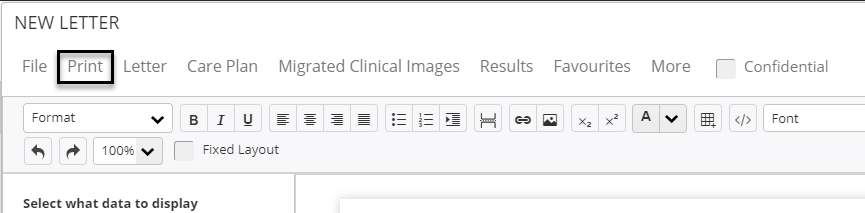
The Print button has been moved from within the More menu, to it’s own button above the letter, to improve the speed of printing letters.
The following fund schedules have been successfully uploaded into Medirecords, and are available immediately.
These changes have come about from customers like you, who have given us their feedback. MediRecords is committed to continuous improvement to allow for ease of use of our product.
See you next month for more exciting new features and functions within MediRecords.

We are excited to announce the recent changes and updates we have released into the Medirecords product. Below you will find a summary of each of the changes we have made.
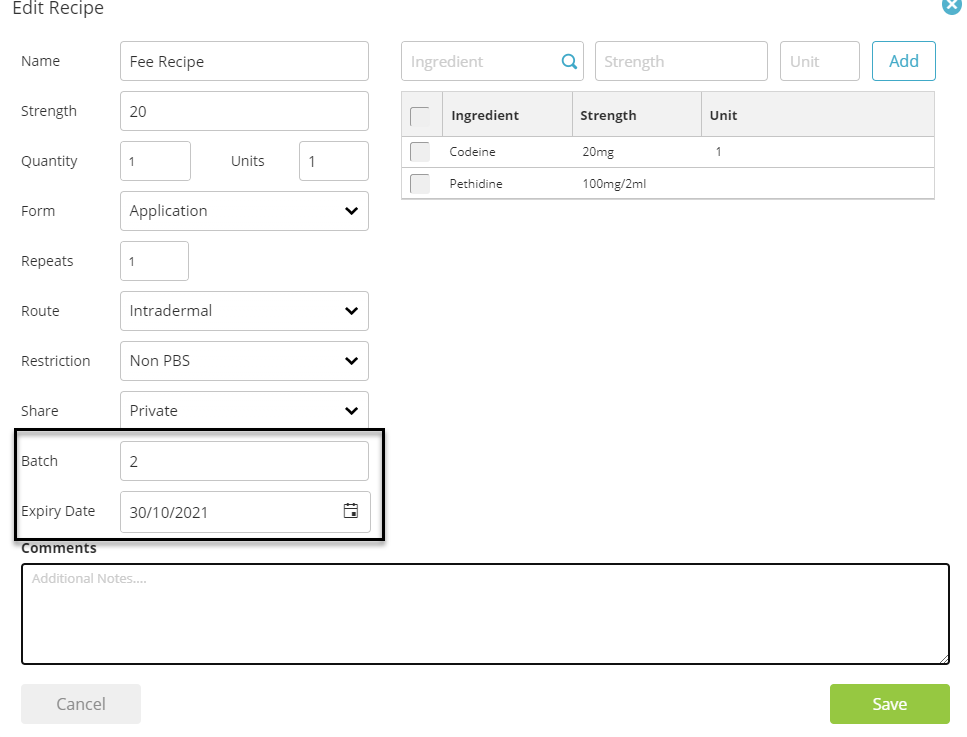
When creating or editing a drug recipe, you may now add your own batch number and expiry. Once a drug has passed the expiry date set within the recipe, you will not be able to prescribe this drug again.
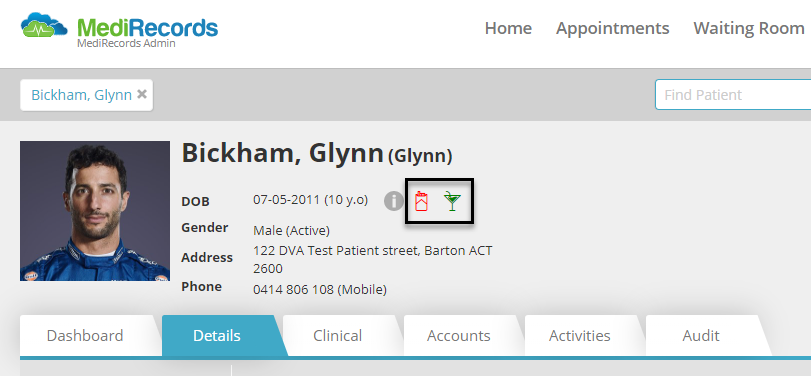
You may now review the alcohol and smoking status of a patient easily, due to 2 new icons added to the patient field. Provided a patient has their alcohol and smoking status recorded within the Tobacco and Alcohol sections of the patient file, these icons will be displayed beside the patient’s date of birth. Hovering over these icons will provide additional information.
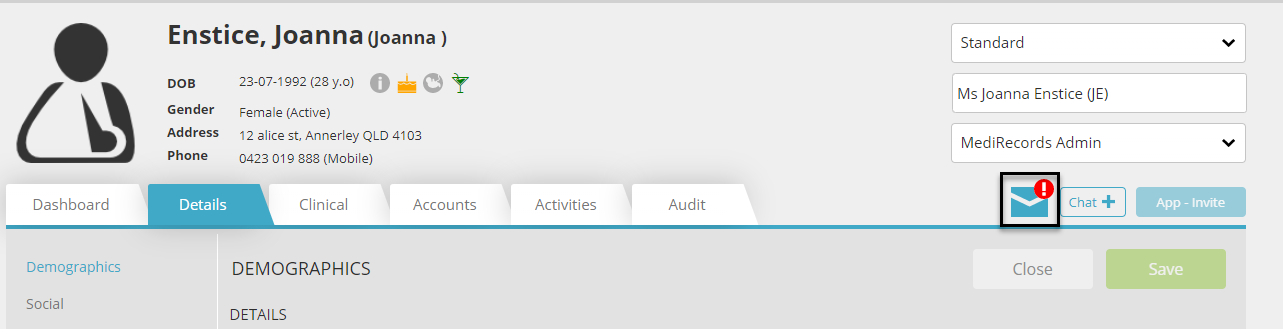
Now when you click on the unchecked mail icon within the patient record, you will be directed to the appropriate result or secure message in question for quick review.
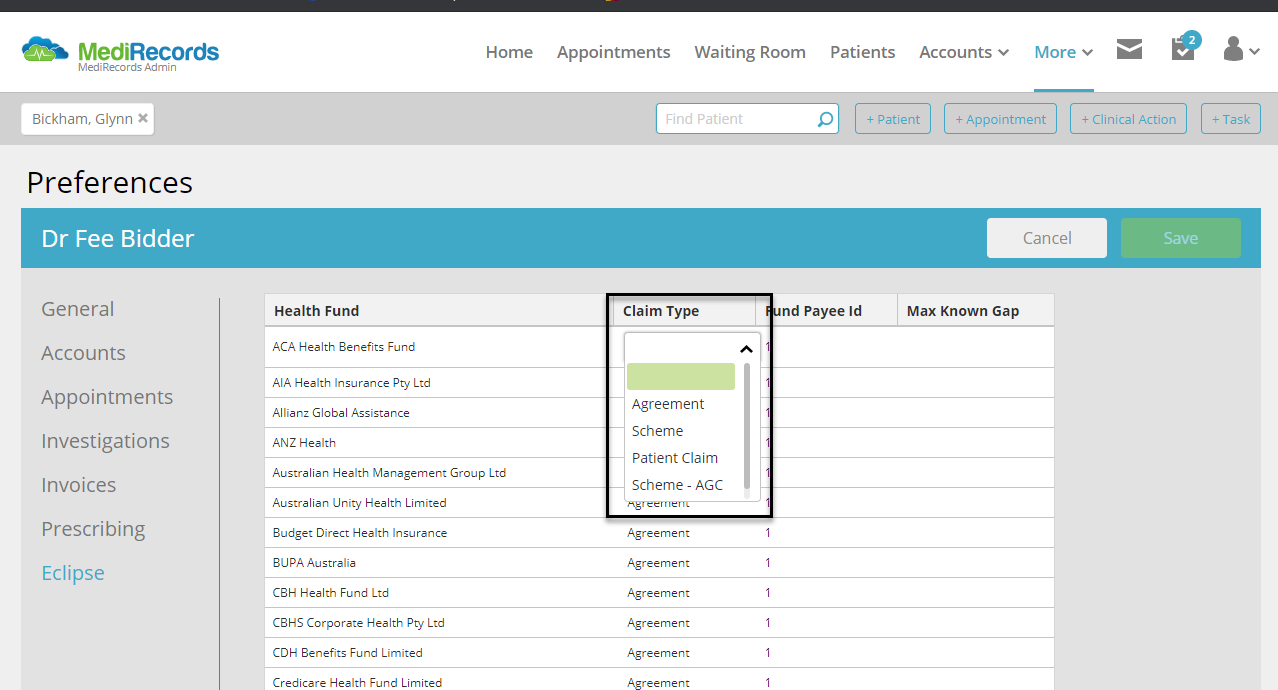
Scheme-AGC has been added as a default claim type within the ECLIPSE configuration window found within Preferences > ECLIPSE. More information on the Access Gap Cover claiming process can be found here: https://www.ahsa.com.au/web/doctors/agc
During July, Medicare released a schedule containing a significant number of item number removals, modifications, and additional items. This has been successfully uploaded into Medirecords, and be used immediately. The majority of the changes were related to Telehealth, Cardiac & Orthopaedic item numbers. For more information on the MBS changes, please view the Medicare website.
These changes have come about from customers like you, who have given us their feedback. MediRecords is committed to continuous improvement to allow for ease of use of our product.
See you next month for more exciting new features and functions within MediRecords.


We’ve also introduced some changes to the way our Appointment Widget supports Telehealth Appointments. These appointments can now be made online and the link for the appointment will be sent to the patient in their confirmation SMS.
Please ensure your Telehealth appointments are configured correctly to appear on your website’s widget.
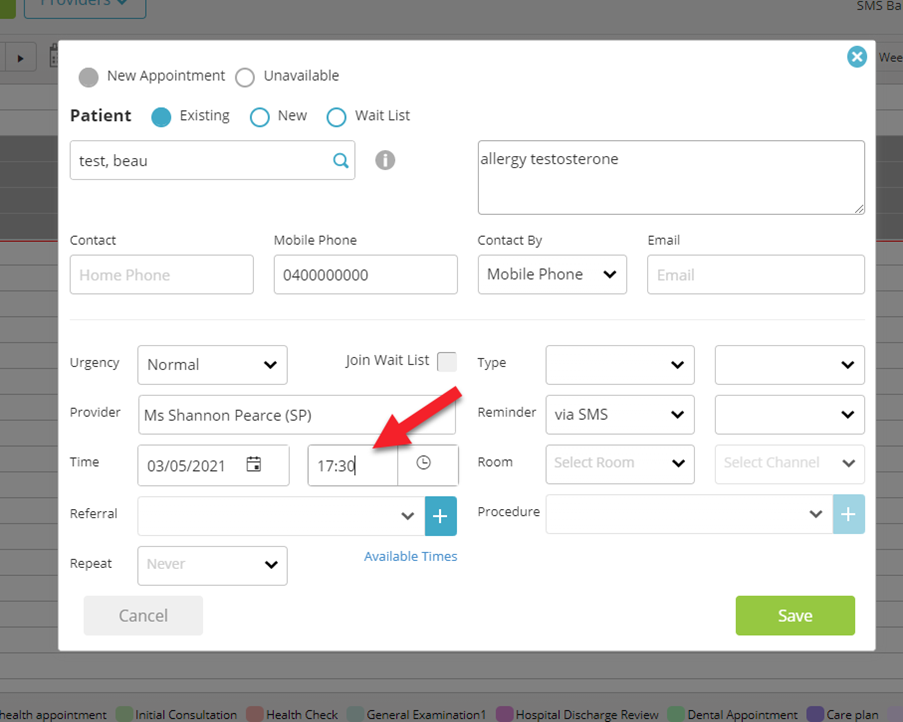
We’ve introduced the ability to free text appointment times when making or editing appointments. The new function lets you type into the appointment time field more specific start times, and also allows you to use 24 hour time which then converts to an AM or PM time in the appointment book.
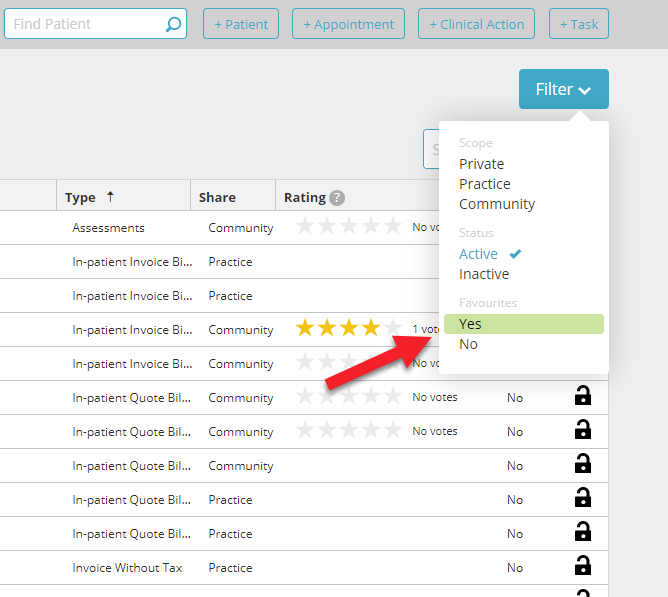
You can now add a filter within the MediRecords Letter Templates search table to indicate that you want to search within your favourites. This will allow you to create a search within only your preferred resources.
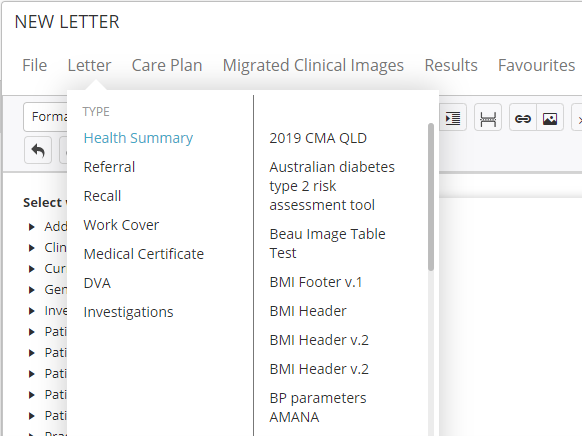
Letters and favourites are now alphabetized in the letter editor, meaning ease of use for our customers.
To allow for greater visibility, two new fields have been added to the Provider Billing Activity Report. ADJ – which shows the amount of adjustments or write offs to the invoice and Outstanding which allows for more visibility of the amount outstanding on the invoice.
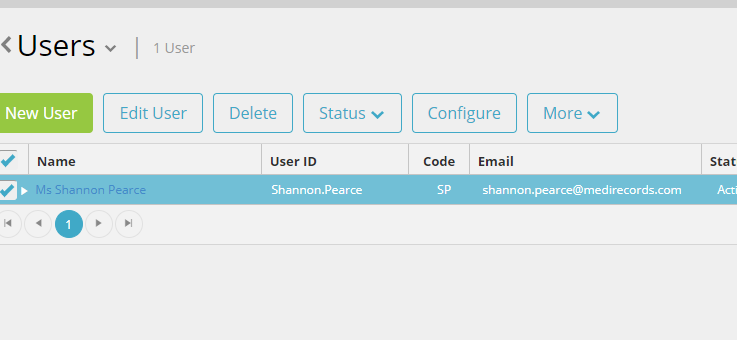
We’ve recently moved the Configure option from the More menu to a button on the sub menu when setting up new users. This will reduce the amount of clicks needed to configure new staff for practices.
Several new fields have been added to the letter writer mail merge library including reason for visit, notes associated with medical conditions including current, past and selected, preferred name and all providers.
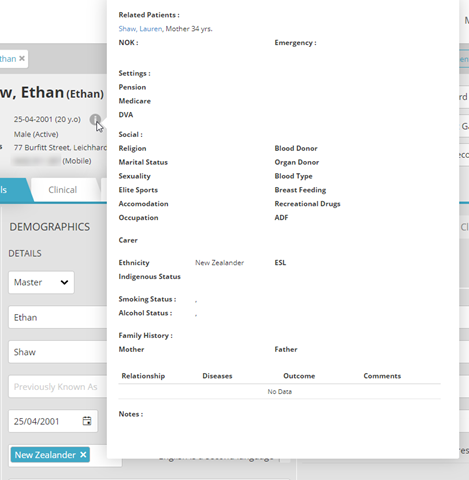
The hover state on the patient header is now shown in full without having to scroll up or down.
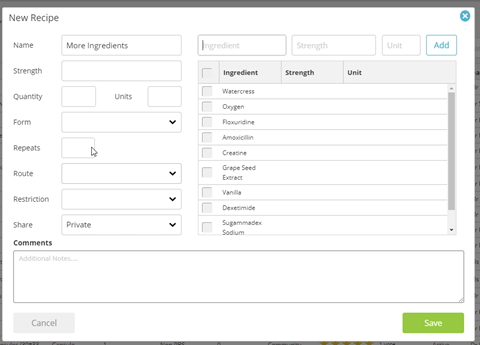
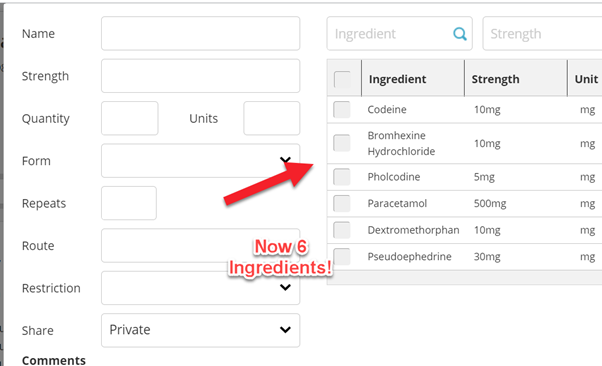
Your custom drug recipes now support more than 6 ingredients.
On the patient record there is now an alert to show if this patient has any unread correspondence in any of the provider’s inboxes. Click here to learn more.

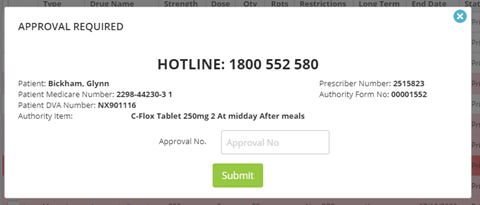
Prescribed authority prescriptions functionality has been improved with additional information now displayed on the approval screen including: Hotline Number, Patient Name, Patient Medicare Number, Patient DVA, Prescriber Number, Authority Form No and Authority item.
These changes have come about from customers like you, who have given us their feedback. MediRecords is committed to continuous improvement to allow for ease of use of our product.
See you next month for more exciting new features and functions within MediRecords.




The mandatory Active Ingredient Prescribing was instated on Feb 1st, MediRecords released its’ new functionality in anticipation of this legislation and user may have found a slight change to their workflows.
Each prescription is now printed with the Active Ingredient of the medication, as well as the brand name if chosen. There are exemptions from the requirement, and the full article can be found on our Knowledge Base here.
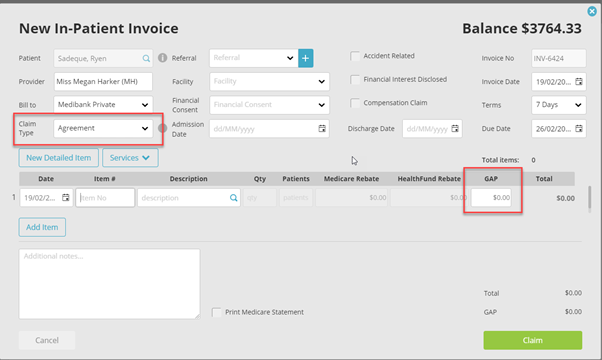
Users can now add GAPs to Agreement invoices to transmit through Eclipse.
Health Funds such as Bupa and HBF only accept claims through the Agreement channel, and prior to this update, a gap was unable to be added onto the invoices transmitted through this channel.
Previously the screen only showed the invoice date for all unbatched invoices in this area, meaning the user needs to click into each invoice to check the date of service. But no more! We’ve updated the screen to also include the date of service as well as the invoice date for ease of use.

Specialists have access to a new report that contains information about their Procedures for a particular date. This can be found in More > Reporting > Patients > Theatre List Report.

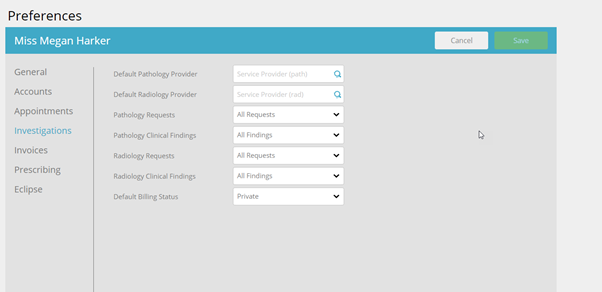
Users can now adjust their preferences for which menu defaults in Investigations between All Requests and their Favourites.
This can be configured in the user preferences.
We’ve made some changes recently to the way resources and contacts are saved in MediRecords.
Previously there were three areas to save your contacts and resources:
We have removed the ability to create Community resources and contacts to reduce the number of items in the grid when searching for these items. Community contacts and templates will only be supplied by MediRecords.
If you have a suggestion or requirement for a resource that would be beneficial for other MR users, please contact the Support Team.
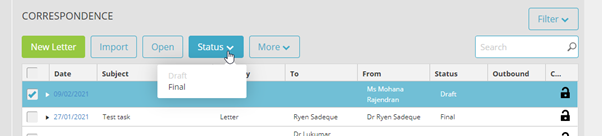
We’ve recently made some changes to the way correspondence is sent to patients via the app. The only correspondence sent to the app will be those that are marked as FINAL. Anything in DRAFT will not be shared.
Did you know MediRecords has the functionality to support multiple patient billing? A function that would assist our users who service Residential Aged Care Facilities or any other clinics that see multiple patients for Medicare or DVA Bulk Billing.
This function can be found in Accounts > Sales, or can be accessed through the patient grid.
Contact our Support Team if you would like more information about Multiple Patient Billing.
For those practices who use Drug Recipes, you may have noticed that the ingredient listing has been extended to 6 ingredients from the previous 4. This should make life a little easier for all our practices who use this function for comprehensive extemporaneous preparations.
This change came about from feedback from a valued customer just like you!
If you need any help with any of these new features, or any others, then please don’t hesitate to contact our friendly support team via email at [email protected], on 1300 103 903 or through the chat function on your MediRecords webpage.


You may have noticed in the last few months that MediRecords have been pumping out new features and updates fairly regularly. Here’s a quick overview of just some of the new functionality, in case you missed anything:
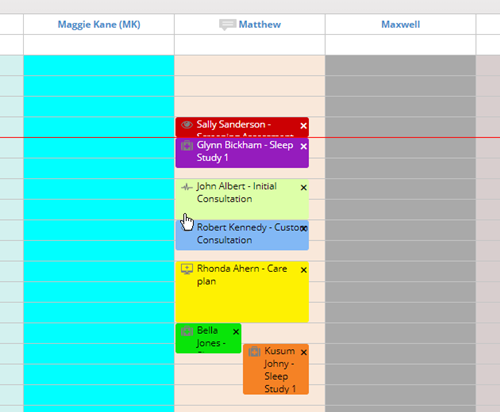
We have introduced vibrant new colours in the appointment book to differentiate between appointment status. These can be seen if you ‘Appointment Colour Palette’ is set to ‘Status’.
The ‘Appointment Type’ is also displayed as text next to the patient name for extra visibility.
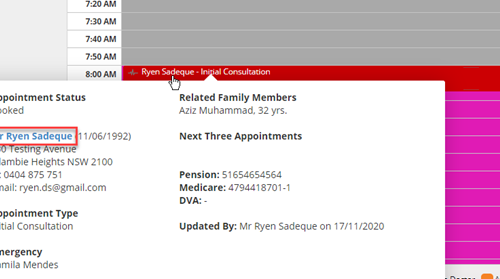
We have also introduced ‘Hover State’. This means you can now see the status of an appointment quickly and easily by hovering the mouse over the appointment.
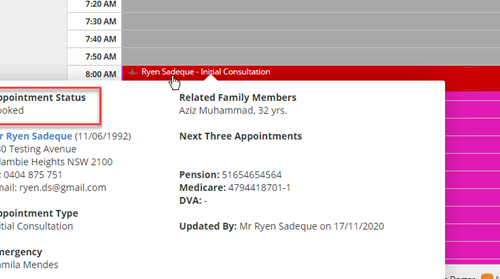
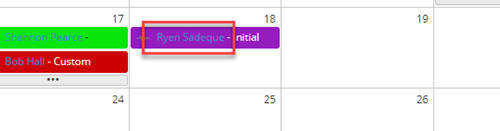
You can now open a patient record from multiple areas of the appointments calendar, just by clicking their name. This feature can be found when hovering over an appointment, when viewing a provider’s calendar by month, and in the Agenda view.
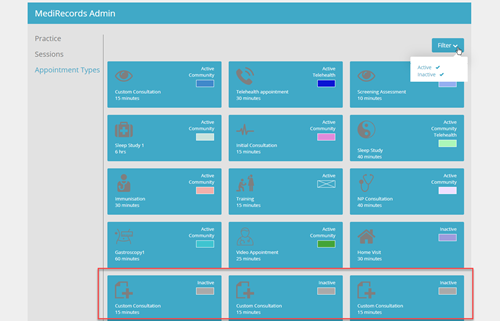
We have also increased the number of different appointment types you can use. Filtering by ‘Inactive’ will reveal the editable tiles, with up to 60 different types of appointments.
You can find out more about editing Appointment Types here.
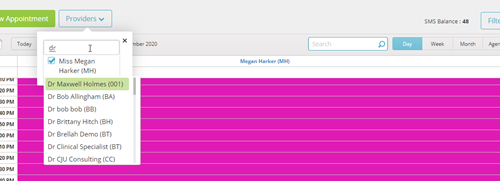
The Provider Filter has been adapted to reduce loading times. You can now easily search and select the providers that you want to see the calendars for by using the search box.
For more information on the Provider Filter and how to set your calendar defaults, see here.
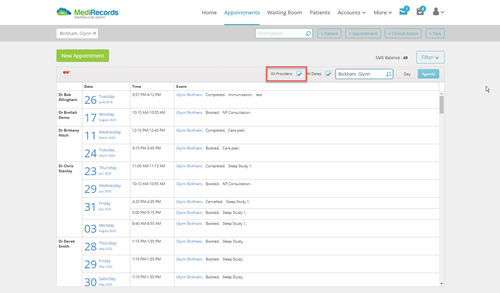
Alongside the Provider Filter, we have implemented improvements to how you search for a patient’s appointments to include an ‘All Providers’ option, if the provider has not already been selected.
This ensures you don’t miss any appointment information.
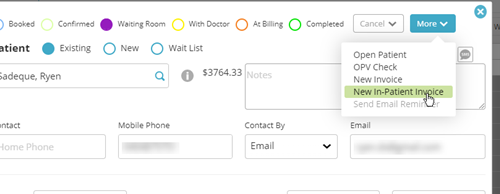
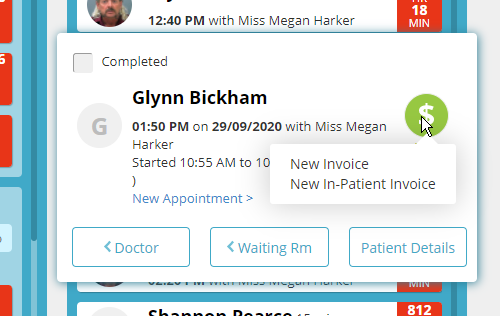
Our in-patient billing functionality has had a huge overhaul and is continuing to be improved.
Health Fund schedules, including AHSA, being updated have been enhanced and derived items are now automatically calculated. We have also removed the automatically populated $400 gap that was being applied to every item, and keep an eye out for the ability to add a Gap payment to an Agreement early 2021. You can now also bill ‘In-Patient Invoices’ directly from the Calendar and Waiting Room.
Additionally, when invoicing from the Appointment screen, the invoice will populate with the service date automatically defaulting to the date of the appointment.
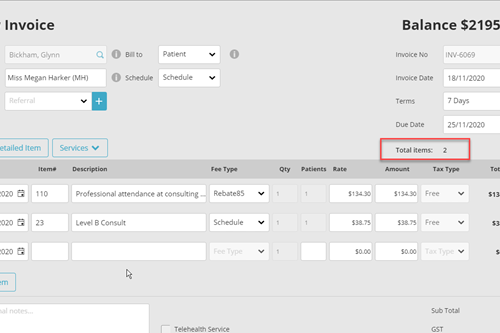
Invoices have been improved to now include number item lines, and an item counter.
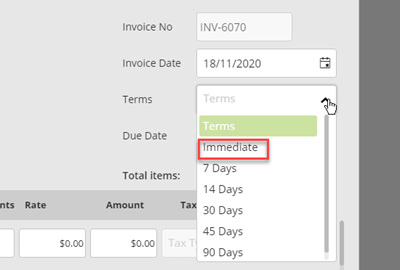
You can also choose ‘Immediate’ in your payment terms.
If you need any help with any of these new features, or any others, then please don’t hesitate to contact our friendly support team via email at [email protected], on 1300 103 903 or through the chat function on your MediRecords webpage.

It may not make you a better GP, but experiencing grief is part and parcel of long-term care, writes Dr Bastian Seidel
Continue reading
Every doctor on the planet is a now a potential publisher
Continue reading