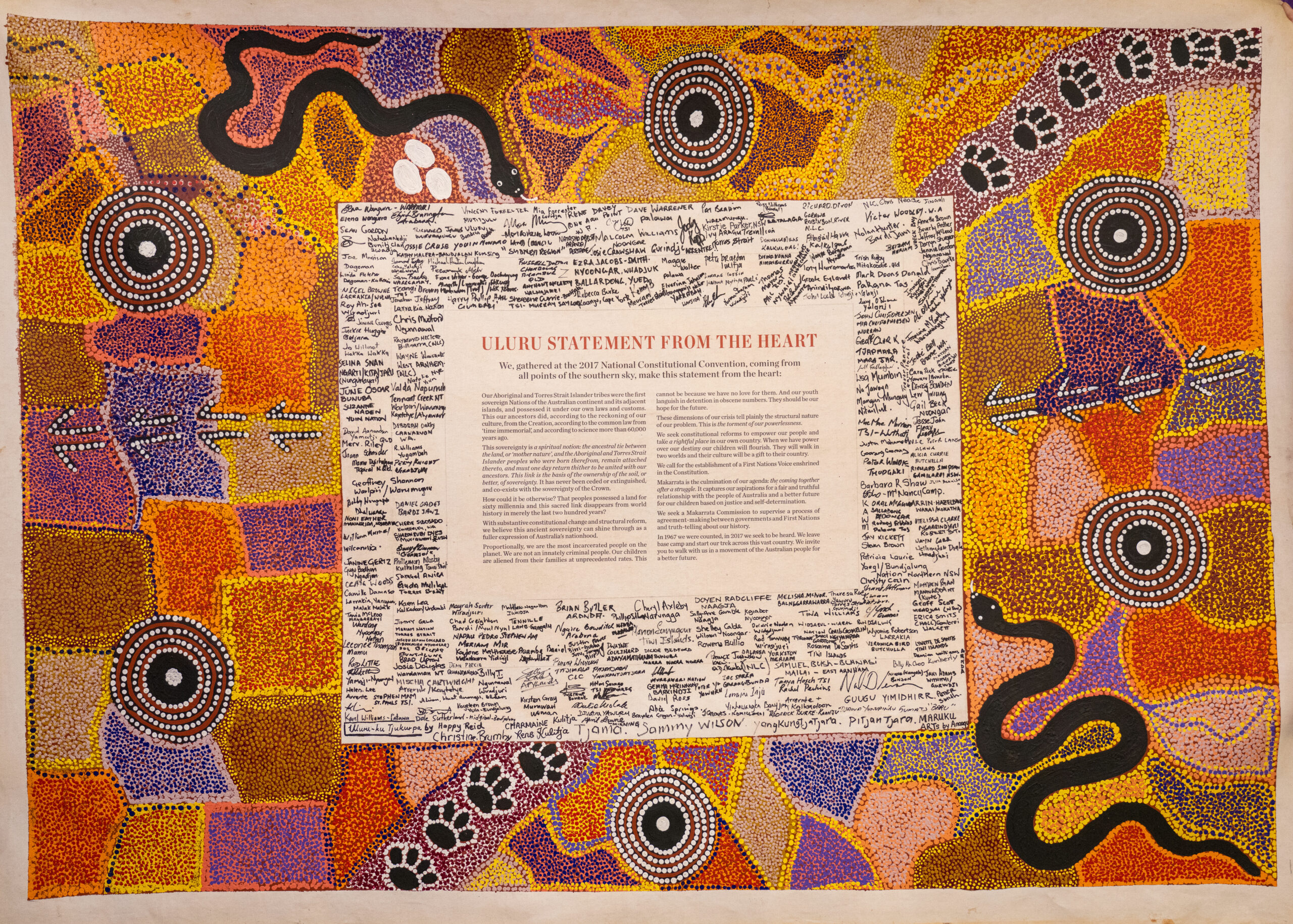
The 2023 referendum is a vote on whether you support the Constitution being changed to establish a Voice to Parliament. You will be asked to answer ‘yes’ or ‘no’ to the following question:
“A Proposed Law: to alter the Constitution to recognise the First Peoples of Australia by establishing an Aboriginal and Torres Strait Islander Voice. Do you approve this proposed alteration?”
If successful, the following words will be added to the Constitution:
Chapter IX Recognition of Aboriginal and Torres Strait Islander Peoples
S 129 Aboriginal and Torres Strait Islander Voice
In recognition of Aboriginal and Torres Strait Islander peoples as the First Peoples of Australia:
1. There shall be a body, to be called the Aboriginal and Torres Strait Islander Voice;
2. The Aboriginal and Torres Strait Islander Voice may make representations to the Parliament and the Executive Government of the Commonwealth on matters relating to Aboriginal and Torres Strait Islander peoples;
3. The Parliament shall, subject to this Constitution, have power to make laws with respect to matters relating to the Aboriginal and Torres Strait Islander Voice, including its composition, functions, powers, and procedures.
As these words show, the proposed Voice does not give Aboriginal and Torres Strait Islander people the power to make, alter or block national laws. The Voice just gives Aboriginal and Torres Strait Islanders a presence in parliament to offer advice and feedback on policies, based on their lived experience.