HepLink Launches Using MediRecords to Expand Hepatitis C Care
March 30, 2026
Media Release
Hepatitis Australia has launched a new national telehealth service designed to deliver unprecedented access to hepatitis C testing and treatment, helping Australia move closer to eliminating hepatitis C as a public health threat.
The service forms part of HepLink, the national hepatitis information and linkage service, and allows people anywhere in Australia to connect with trained nurses, streamlined care pathways, and rapid access to treatment via telephone and virtual care.
Powered by MediRecords’ secure cloud technology and the Coviu telehealth platform, HepLink enables Australians to receive testing guidance, arrange blood tests, access clinical consultations and, where appropriate, receive prescriptions for curative hepatitis C treatment, without needing to attend an in-person appointment.
Hepatitis Australia CEO Lucy Clynes said the new service builds on the extraordinary progress Australia has made since hepatitis C cures were made widely available through the Pharmaceutical Benefits Scheme in 2016.
“More than 100,000 Australians have now accessed treatment and almost 100,000 have been cured of hepatitis C. That is one of the most significant public health achievements in a generation.
But around 63,000 Australians are still living with hepatitis C and many are unaware they have it or are not currently connected to care. HepLink helps close that gap by making testing, treatment and expert support easier to access from anywhere in the country.”
Lucy Clynes, Hepatitis Australia CEO
Digitally enabled care pathway
The HepLink telehealth service is supported by secure cloud-based clinical technology from MediRecords and its Engage patient portal, integrated with the Coviu telehealth platform and AI Scribe technology, enabling an end-to-end digital care pathway for patients.
Through the system, nurses and clinicians can securely manage patient records, share information and education materials, arrange testing, conduct telehealth consultations and issue ePrescriptions where appropriate.
This digitally enabled workflow allows people to move from their first enquiry to treatment initiation through a streamlined virtual care model — removing barriers for those who may struggle to access traditional health services.
Alongside Canada, Australia is now among the only countries to offer a nationwide telehealth service of this kind.
HepLink also supports general practitioners who may be unfamiliar with hepatitis C treatment, offering guidance and referral pathways to ensure patients are not left untreated.
MediRecords CEO Matthew Galetto said digital health platforms play a critical role in expanding access to care for people who may otherwise fall through the cracks.
“Digital care models are essential to reaching patients who may not present through traditional healthcare pathways,” Mr Galetto said.
“By supporting HepLink with secure cloud infrastructure and integrated telehealth capability, we’re helping enable a scalable national approach to hepatitis C care.”
Matthew Galetto, MediRecords Founder and CEO
Supporting Australia’s elimination goal
Australia has made major progress toward eliminating hepatitis C since the introduction of direct-acting antiviral treatments in 2016.
Since then:
The number of Australians living with chronic hepatitis C has fallen by more than 60 per cent
Deaths among people living with hepatitis C have declined significantly
Almost half of treatments are now prescribed in primary care settings, improving access across the country.
However, treatment rates have slowed in recent years as remaining patients are harder to reach.
HepLink is designed to reconnect those individuals with care by providing confidential, easy-to-access support and clinical guidance.
Ms Clynes said initiatives like HepLink will be essential if Australia is to achieve its goal of eliminating hepatitis C.
“We now have the tools to cure hepatitis C quickly and safely,” she said.
“The challenge is ensuring people know about the cure and can access care when they need it. HepLink helps ensure no one misses the opportunity to be tested and treated.”
How to access HepLink
Anyone in Australia can access the HepLink service by calling 1800 437 222 or visiting www.heplink.au.
The service provides:
Information about hepatitis C testing
Support to arrange blood tests
Virtual clinical consultations where required
Access to prescriptions for curative treatment
HepLink is the national hepatitis information and linkage service operated by Hepatitis Australia in partnership with community hepatitis organisations nationally. HepLink is funded by the Australian Government Centre for Disease Control.
The HepLink telehealth service is made possible through a community grant from Gilead Sciences Australia.
MediRecords and Coviu are proud to support this vital healthcare initiative.
Why choosing a Practice Management System shouldn’t be a marriage for life - but neither should it be married at first sight
March 10, 2026
by Tim Pegler
Choosing a Practice Management System (PMS) is not a decision to take lightly.
Like a significant other, a PMS needs to be dependable, adaptable, and easy to spend time with. It should be open to growth, including making new connections. It should not be stuck in the past.
However, for time-poor clinicians their clinical software is all too often a set and forget decision. It’s the equivalent of ‘til death do us part’ (or the servers need replacing). Until then, inertia wins the day.
Fortunately, Australian healthcare is at a crossroads. There’s never been a better time to review technology partnerships, following Federal Government confirmation the future of healthcare is cloud-first and FHIR-enabled.
This doesn’t mean it’s time for a software swingers party or a married at first glance impulse buy. Migrating to a new Practice Management System can be complicated. Here are six things to consider carefully if you’re ready to reconsider your pairing:
1. Technology is evolving. Your PMS needs to keep pace
The Federal Government preference for cloud-hosted technology with FHIR (Fast Healthcare Interoperability Resources) connectivity is pragmatic and based on worldwide trends. There are rising expectations for data to be shared from Primary (e.g. GP) to Tertiary (e.g. hospital) care organisations in real time because communication silos create risk. Consumers increasingly expect access to their data – and their doctors – wherever they are. Your technology needs to support this with secure integration to government systems. Ask your vendors:
What security certifications do they have?
Are they conformant with government regulations for prescribing safely?
How often do they release product updates and how easy are these to install?
What’s on their roadmap?
2. Scalability is not negotiable
Growth looks different for every organisation. You might:
Add multidisciplinary teams for holistic, shared care
Expand to multiple sites
Provide a combination of face to face and telehealth care
A scalable PMS accommodates growth rather than impeding it. This is why cloud systems have become the modern standard; they scale effortlessly, securely, and cost effectively.
3. Remote workforces are here to stay
The pandemic changed healthcare forever, resulting in workforce casualisation, proliferation of virtual care services, and teams working from anywhere with Internet access. Your preferred PMS needs to be limber enough to support:
Telehealth consultations
Distributed administrative teams
After hours clinical care
Offsite reporting, billing, and triage
Multilocation collaboration
If your workers are grinding away via legacy remote desktop systems, you’re likely to be losing time, money and team morale.
4. API connectivity is essential
API and FHIR interoperability enable innovation. Look for a PMS technology partner with open, well documented APIs ensuring secure connection with:
A wedding costs more than a dress, rings, catering and flowers. Factor in photography, suits, vehicle and venue hire, celebrants, music, and so much more. Licence fees for a server-based or hybrid PMS may be attractively low, but you need to budget for desktop downtime and IT support for managing your back-ups, software updates and security patches, not to mention the hardware, building and utilities expenses for owning, running and cooling servers. A server is a short-term investment; you’re committing to $40k or more, each time you replace the hardware. You also need to dispose of it securely and, ideally, sustainably.
Cloud PMS systems mean you can ghost server issues, swipe left on IT contractors and let your technology partner automate software management for you.
6. Where do you see yourself in a decade?
People change. So does the healthcare sector. Hospital-, aged-, and palliative care will increasingly be delivered at home, to maximise patient comfort and convenience, and minimise costs. Can your nursing teams deliver patient care wherever they need?
Actively seek PMS software with the flexibility to satiate new needs as they arise.
If it’s not marriage for life, what is it?
Think of your PMS as a long-term partnership, built on performance, adaptability, and trust.You shouldn’t feel trapped by it. You shouldn’t choose it impulsively. You should feel confident it’sthe right pairing for today and tomorrow. If it’s cloud-based, scalable, FHIR-enabled, and API-driven, that’s a lot of green flags.
Moving forward
If you’re considering opening a new business, MediRecords’ Complete Medical Practice Startup Blueprint provides a comprehensive checklist on things to work through.
If your existing business is looking for a new technology partner, please book a call via [email protected] so we can discuss your requirements.
Opening a medical practice involves more than finding a location and hiring staff. From Medicare compliance to digital health registrations, there are many steps to get right.
We’ve simplified the process into a practical checklist to help you launch a modern, compliant clinic with confidence.
Predictions and peer pressure in the AI playground
January 21, 2026
by Tim Pegler
For a few years now I’ve dusted off my crystal ball each January, gazed into its misty depths, and asked, ‘What will change in digital health in the 12 months ahead?’
This year it felt pointless asking as all the omens point to obvious answers. I didn’t need to be psychic to predict AI and cyber security would dominate developments in healthcare in 2026.
And then the ground shifted, possibly seismically. AI giants OpenAI and Anthropic formally launched healthcare initiatives and the aftershocks have begun. So, hot on the heels of the announcements, let’s look at what the big five AI platforms are doing in health:
OpenAI’s ChatGPT
Watch how your friends and family get their health information now. If they’ve dumped Dr Google in favour of a ChatGP(T), they’re part of a mass migration. It’s estimated that 5% to 25% of ChatGPT searches now relate to healthcare, so it’s no surprise OpenAI is cementing its role in health.
OpenAI’s January 8 announcement said ChatGPT Health will be a consumer-facing information and assistance tool where you can upload results and ask questions, draft clinical documents, review research and summarise data. In the US, personal health records can be connected via middleware, to analyse progress. Major training tools, like MyFitnessPal and Peloton, are looking to integrate with ChatGPT.
For large healthcare organisations, ChatGPT for Healthcare promises a HIPAA-ready workspace, focused on administrative efficiency. It can be integrated with an Electronic Medical Record (EMR) to boost automation, clinical decision support and planning. Major hospitals are already proceeding to pilot implementations.
ChatGPT Health is available to a limited user group in Australia, with broader access likely from next month.
Anthropic’s Claude
Claude for Healthcarelaunched on January 11 with beta products for enterprise and consumers. At present, these are limited to US subscribers, with no timeline for entering the Australian market. On the consumer side, Apple and Android integrations will enable sharing of health histories, results, and wearable device data with Claude. Claude says this will enable detection of patterns, “more productive conversations with doctors” and humans who are better informed about their health.
At enterprise level, Claude is also HIPAA-ready and aligning with major databases such as PubMed, the international Classification of Diseases (ICD-10) and the US system detailing medical billing codes.
Microsoft’s Copilot
Microsoft announced its health AI push early and has the advantages of being pre-installed in many computers. Copilot for Health identifies as a consumer-friendly ‘AI Companion’ that draws on medical journals, especially Harvard Medical School resources. It can provide symptom and wellness information and point you toward nearby health services, (hopefully with available appointments).
At EMR level, Microsoft’s play is through Dragon Copilot for medical professionals (no known Australian release date) and enterprise documentation tools under the Microsoft for Healthcare banner.
Google’s Gemini
Google has research tools and enterprise cloud platforms in its armoury. The former includes Med-Gemini, which can assist with medical exam preparation, clinical reasoning and patient file analysis, and MedGemma which is used with diagnostic imaging, medical devices and other clinical documents. Finally, Personal Health LLM (looks like the marketing team haven’t got to this one yet) will coach consumers based on data from devices like Fitbit.
At enterprise level, Google has Vertex AI Search for Healthcare in EHR systems and MedLM for documentation, scribing and clinical coding. Hospitals using Google Workspace will likely use Google AI tools.
Google’s Health Connect is also promoting FHIR (Fast Healthcare Interoperability Resources) standards to improve interoperability of health information sources.
Beyond these initiatives, Google Health is a leader in deep dive medical research and drug development.
Perplexity
The other big AI player, best known for its comprehensive referencing, hasn’t announced a formal healthcare move. Partnered with large research libraries like Wiley, Perplexity promises an “AI research and productivity layer” but lacks AI scribe features or options for EMR integration.
Peer pressure
With Claude, Copilot and Perplexity licensing respected sources of peer-reviewed research, it’s clear that attribution and credibility are invaluable to AI platforms. It’s also obvious everyone is nervous about being a global test case for inaccurate, dangerous, or deadly “hallucinated” data. The platforms all warn they are not diagnostic in nature; they ‘inform’ but cannot substitute for advice from qualified medical practitioners. And they can all make mistakes.
In the interests of objectivity, I asked each of the five tools to discuss the pros and cons of their peers, versus themselves. The findings were remarkably consistent:
Claude won plaudits for ethics, safety, privacy controls and clinical reasoning but was marked down for US-centric data and limited interoperability.
Gemini had the advantages of deep learning from Google search tools and medical research, along with software omnipresence.
ChatGPT has market maturity and mass usage, but this comes with a perceived higher risk of hallucination.
Copilot scored for being a handy administration and documentation tool embedded in hospitals. That was a back-handed compliment; for clinical reasoning, Claude and Gemini were the go-tos.
Perplexity was nominated as the best place for doctors to verify information and perhaps the least likely to hallucinate.
Dance partners
The other battleground is for data partners. Alliances with the developers of phones, wearables, health apps, medical devices, fitness and rehabilitation equipment, and clinical trials, will be critical. Primary care practice management systems might even come under the microscope.
Doing it Down Under
Australia is significantly smaller than the US and lagging on data interoperability, (despite the best efforts of FHIR-friendly vendors like MediRecords.) Just like we don’t see new features for Apple Watches for months or years after they’re released, the new AI platforms may face regulatory reviews and other hurdles Down Under.
One thing is clear. The Therapeutic Goods Administration (TGA) will be watching to see if they stray into diagnostic device territory.
MediRecords Evolve is our growing suite of agentic AI tools designed to expand the clinical and admin capabilities of your practice, while saving time and minimising the risk of human error.
Reduce your workload today, and increase your capacity with every new release.
MediRecords unveils Evolve Direct, an AI-powered inbox management solution.
December 10, 2025
Media Release
MediRecords today announced the upcoming launch of Evolve Direct, an innovative AI-powered tool designed to streamline medical clinic inbox management and dramatically reduce administrative burden, scheduled for release in early 2026.
For many clinics, managing incoming documents has been a time-consuming, manual process. Staff have traditionally downloaded documents from external inboxes, located the correct patient, and uploaded files into the clinical system—a repetitive workflow prone to human error.
Evolve Direct changes everything.
Leveraging advanced AI technology, Evolve Direct automates the entire process:
Analyses and classifies incoming documents
Assigns the correct provider
Matches documents to the right patient record
Performs automated virus scanning
Directs unmatched documents to a Holding Bay for review
This means clinics can simplify the current manual 18-click process to just three clicks, saving time, reducing risk, and improving accuracy.
Beta testing with existing clients has shown the following benefits:
Significant time savings
Early feedback from test clinics with up to 10 doctors shows potential savings of up to 120 minutes per day, equating to:
10 hours per week
40 hours per month
480 hours per year
Major reduction in manual effort
Previous workflow: ~18 clicks per document
Evolve Direct workflow: 3 clicks
That’s an 83% reduction in manual steps, fewer touchpoints, and less cognitive load for staff.
Improved accuracy & reduced risk
Eliminates manual download/upload errors
AI ensures correct provider assignment and accurate patient matching
Faster classification means results and correspondence reach the right person sooner
Enhanced security
Built-in virus scanning protects against malicious attachments
Reduced human handling improves privacy and compliance
Scalable for growth
As document volume increases, Evolve Direct absorbs the workload without adding pressure to admin teams, supporting sustainable business growth.
MediRecords founder and chief executive officer Matthew Galetto said the launch demonstrates a commitment to simplifying clinic workflows to reduce burnout and boost patient care.
“Evolve Direct provides a significant boost for clinics under increasing cost and time pressures. By largely automating inbox management, we’re helping practices reclaim hours each week, reduce risk, and focus on delivering quality care.”
Matthew Galetto, MediRecords Founder and CEO
Building a multi-agent AI future for healthcare
The launch of Evolve Direct is part of MediRecords’ broader strategy to introduce a suite of specialised AI agents that lift efficiency, accuracy, and quality across clinical and administrative workflows. MediRecords has already deployed Evolve Patient Summary, an AI agent that rapidly distils a patient’s record into a clear, usable snapshot for clinicians.
More agents are planned. Each will draw on MediRecords’ position as the patient system of record, unlocking rich clinical data and automating time-heavy tasks so practices can operate with greater confidence, speed, and scale. Evolve Direct is the next step in that journey, with further AI-driven tools set to roll out through early and beyond.
To sign up for early information and launch updates for Evolve Direct, sign up below.
Too many apps on the dancefloor: digital continuity, governance and productivity 101
26 November 2025
Do we try to sew together a mass of emerging apps to connect and refer up and downstream, or use agile platforms that can connect it all in one system?
The federal government has drawn a line in the sand: since October 2025, pathology providers must upload reports to My Health Record by default, with diagnostic imaging following in February 2026. Medicare benefits are only payable when organisations comply.
That’s just the beginning.
The government is explicitly exploring ways to expand default sharing beyond pathology and diagnostic imaging to other types of key health information, including discharge summaries, specialist letters, and care plans.
It’s not a question of if GP consultations, specialist visits, and allied health services will face the same requirements. It’s when.
And it’s not just about uploading data. Since 2023, clinical software that connects to My Health Record has been required to meet mandatory security conformance standards.
While the government ultimately stopped short of mandating full Essential Eight compliance (recognising that very few systems would have met the threshold), the direction is clear: minimum cybersecurity standards are coming as a prerequisite for exchanging information with government services, including Medicare.
If your systems can’t demonstrate baseline security resilience, you won’t be connecting to national infrastructure much longer.
For organisations managing both internal health services and external community referral networks, this integration challenge isn’t theoretical. It’s the difference between being able to answer an auditor’s questions and hoping they don’t dig too deep and it’s a massive potential pivot to or away from productivity.
When audits expose the integration gap
The Australian National Audit Office’s recent audit of Defence health services put numbers to what many already suspected: poor integration between clinical and financial systems made it impossible to reliably track what services were delivered, by whom, or whether claims matched care.
Defence is far from unique.
The same pattern shows up across corporate health services, corrections health, employee assistance programs, and anywhere else an internal health service refers patients to external community providers.
What the audit exposed was that when you refer internally and deliver externally without a unified system, you lose the thread. You can’t track the referral pathway. You can’t validate service delivery. You can’t reconcile the claim back to the original clinical decision.
When the referral chain breaks
A patient visits an internal health service. The GP refers to a community specialist. The specialist orders pathology and refers to allied health. Someone else handles the follow-up. Each provider bills separately, through separate systems.
By the time finance tries to reconcile it all, tracking the chain of referrals feels more like forensic investigation than accounting. Clinically coded data lives in one system. Community provider billing happens in another. Medicare bulk bills go through one channel, private providers through another, and DVA or other contracted arrangements follow their own logic entirely.
When something doesn’t add up (and it often doesn’t), you’re left hunting through emails, spreadsheets, and disparate databases trying to reverse-engineer what actually happened.
For organisations with duty-of-care obligations, where you’re responsible for health outcomes even when care is delivered externally, that lack of visibility is a significant governance failure. But it’s one we’ve largely lived with because our systems haven’t been sophisticated enough to cope with the problem.
However, now that we can contemplate a system that doesn’t just connect these elements but in doing so also creates an audit trail, it’s not just governance people should be thinking about. It’s productivity.
How much money and workforce productivity will start to emerge in our healthcare system when we start properly joining up all the elements of referral, clinical record, booking and invoicing, in real time?
We are literally talking in the billions. Yet it’s something people haven’t largely even contemplated in the current digital transformation of our healthcare system … yet.
How it should work
If your internal health service already uses a platform that manages referrals, clinical documentation, billing, and compliance, extending that same platform to community providers creates an unbroken chain of accountability from initial consultation to final payment.
Internal service creates a referral. The system captures the clinical justification, authorised services, and any service limits. The community provider receives the referral, accesses the same system, sees the referral context, and documents their service delivery. Service is coded and billed. The system automatically validates that the service matches the referral authorisation. Finance reconciles in real-time. Because everything lives in one system, there’s nothing to reconcile manually.
Every action connects to the one before it. The audit trail is automatic. The organisation maintains visibility and governance over care delivered externally, without sacrificing provider autonomy.
But the system pay-off is in productivity of the provider and the patient. Literally millions of hours not wasted in trying to connect the dots on payments, invoicing and bookings.
The pay-off is for everyone but providers will need to be able to extend the system they use internally to their external provider network.
Some systems today are starting to claim they can do this. But most only offer elements of solving the problem.
A cloud-based e-referral system, for instance, is neat but it can’t seamlessly integrate to bookings and invoicing in a line to create a single audit trail and set of invoices. These are nice-to-have new elements but they are essentially modern versions of the old SMD systems.
Solving the referral-to-community problem
Forgive me here but I’m going to talk about the one system I’m involved with, MediRecords. I’m doing this because I know it so well, it provides a great example of what is achievable if you are able to extend your system seamlessly to external provider networks and, well, I’m selling it, obviously.
Surprisingly, given the seismic productivity gains on offer for both patients and providers, systems like MediRecords – essentially an FHIR-enabled cloud-based EMR with lots of good APIs – are, so far, few and far between in Australia.
For a long time the government has not really incentivised cloud-based connectivity in Australia with the result that many old server-bound integrations have been able persist a long time in the system.
Other cloud-based systems like MediRecords with longitudinal system connectivity capability do exist, but I’ll let you do that research.
What’s important is these new core cloud systems are agile in their ability to connect and share data in real time with other systems, which is auditable and which, because of the flexibility of connection, provides the ability for all elements of a single patient transaction to be captured and processed.
Where MediRecords is already deployed as the core system for internal health services, extending it to community providers means those providers gain access to the same platform, but with appropriate scope limits and data access controls.
A community GP sees only their own patients and referrals, but the referring organisation maintains oversight across the entire care pathway.
The platform handles referral management with structured referrals including clinical context, service authorisation, and validity periods. It manages multidisciplinary workflows with different claiming rules for GPs, specialists, allied health, pathology, and imaging. Real-time compliance happens automatically, validating services against referral authorisations and payor rules. And every referral, service, and claim comes with audit trails that prove clinical appropriateness.
For enterprise and community networks managing dozens of sites and hundreds of external providers, dashboards show where referrals are flowing, where services are getting stuck, and where revenue patterns don’t match clinical expectations.
Meeting regulatory standards
MediRecords supports FHIR and OntoServer standards, integrates with national infrastructure via secure messaging, and stores the structured data required for My Health Record uploads.
Under the hood, MediRecords is built with double-entry accounting, a general ledger, and full journal management. This provides the financial backbone that government finance departments and enterprise systems require.
MediRecords’ cloud-native architecture aligns clinical and financial assurance with enterprise-grade security. For organisations evaluating community provider networks, that means one less integration risk and one less compliance gap.
The trade-off: Integration v independence
When you’re managing thousands of services, including external referrals across hundreds of providers, manual review is almost impossible.
Some advanced providers, MediRecords being one of them, are exploring how artificial intelligence can automatically identify, link, and map services to item codes, validate claims against payor rules (whether government, insurer, or contract-based) and flag services that don’t match referral authorisations.
That means fewer manual audits, faster reconciliation, and better confidence that community providers are claiming appropriately. The result is a platform that doesn’t just capture data. It learns from patterns and helps organisations maintain governance without drowning in manual review.
What comes next
Health reform is heading in one direction: integration, data sharing, accountability and significant productivity gains, particularly in the area of workforce.
Organisations responsible for health outcomes are being asked to demonstrate traceability even when care is delivered externally and solve their productivity and workforce issues. That’s now just not feasible with legacy systems: when internal services and external providers use completely different platforms.
The path forward isn’t more integration layers, one-off cloud-based connection applications or complex data feeds. It’s system continuity.
Using the same platform internally and externally, so that clinical accountability, financial governance, and regulatory compliance flow naturally across organisational boundaries.
For organisations already using MediRecords internally, extending it to community providers isn’t just the path of least resistance. It’s the path of greatest assurance and productivity.
Connected care, credible claims, real compliance and generationally impactful productivity gains.
That’s what modern health governance and productivity looks like when care crosses organisational lines, which more and more these days it must if we are to manage a system rapidly moving to team based chronic care management.
MediRecords Premium launches Clarity: Business intelligence tools to unlock efficiency and value in healthcare
November 20, 2025
Media Release
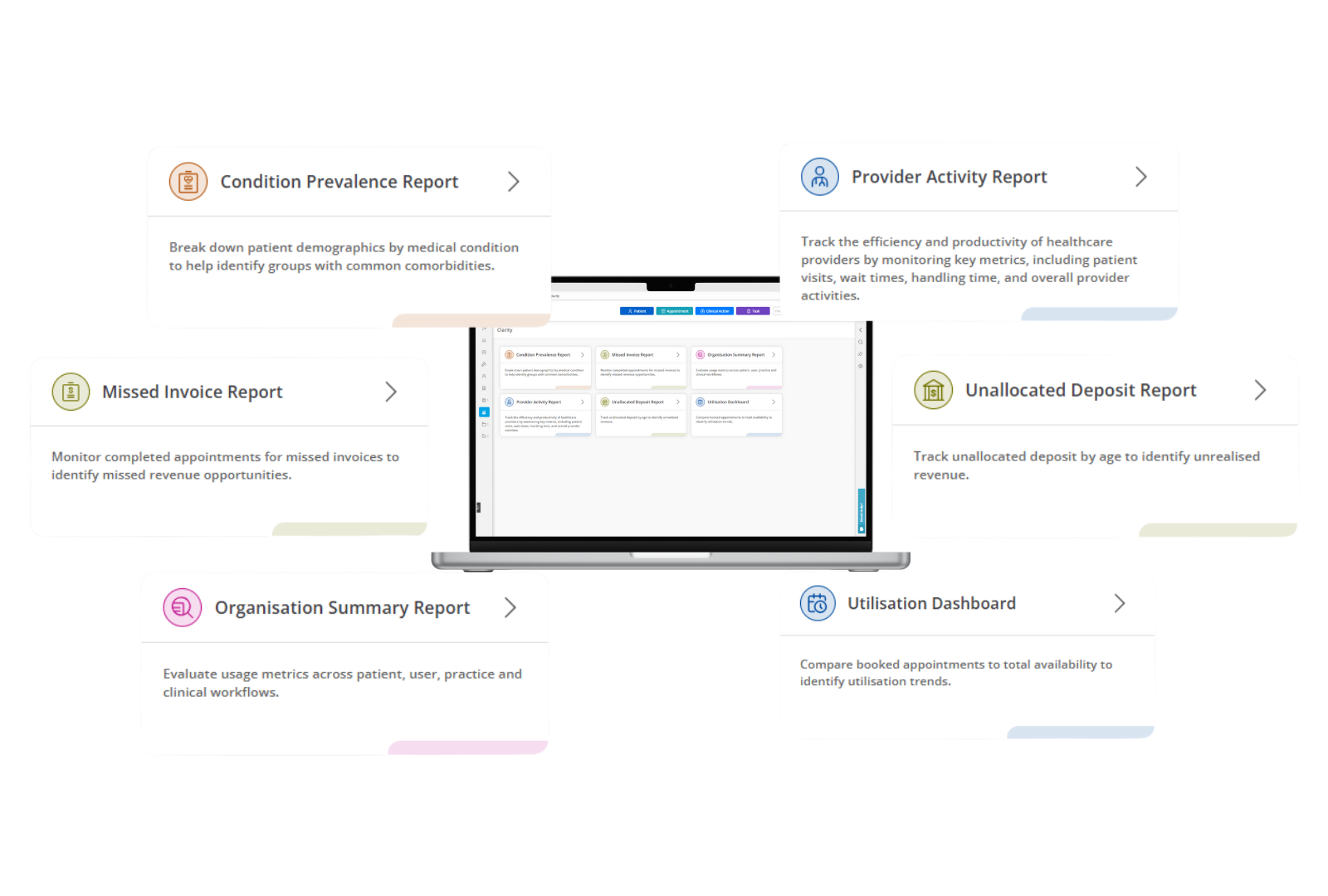
MediRecords has introduced Clarity, a powerful new business intelligence solution designed to help healthcare organisations uncover hidden revenue, optimise workflows, and make data-driven decisions faster. Built into the MediRecords Premium platform and powered by Qlik Cloud, Clarity delivers up-to-date dashboards and analytics that transform operational visibility into actionable insights.
Healthcare organisations face mounting pressure to improve efficiency and financial performance. Missed invoices, unallocated deposits, and opaque billing patterns can erode revenue and compromise care quality. Clarity addresses these challenges by providing organisation-wide visibility, enabling teams to identify gaps, recover lost income, and enhance productivity.
Clarity’s initial suite of dashboards includes: up
Missed Invoice Report
Detect and recover lost revenue opportunities.
Provider Activity Report
Gain insight into staff billing patterns and productivity.
Unallocated Deposit Report
Track and reconcile payments efficiently.
Condition Prevalence Report
Inform preventative care strategies.
Organisation Summary Report
Monitor performance across sites.
Utilisation Report
Measure resource use and optimise scheduling.
“We know our clients value actionable data insights, and Premium is a great way to delve deeper into business efficiency. We’re also pleased to add new tools supporting team care, helping organisations deliver more connected and collaborative healthcare.”
Matthew Galetto, MediRecords Founder and CEO
Clarity is part of MediRecords Premium, which also includes advanced tools for case management, group appointments, global requests, and custom fields – all designed to support connected, multi-disciplinary care.
To find out more, visit the MediRecords Premium website.
MediRecords partners with General Practice Registrars Australia to support the next generation of GPs and RGs
November 5, 2025
Media Release
General Practice Registrars Australia welcomes MediRecords’ support for the next generation of GPs and RGs
General Practice Registrars Australia (GPRA) has announced a new partnership with MediRecords, offering GPRA members exclusive discounts and access to Australia’s leading cloud-based clinical and practice management software.
The collaboration will support the next generation of doctors as they build their careers and future-proof their practices with a digital platform that travels with them.
MediRecords enables GPs and Rural Generalists (RGs) to securely access patient records from anywhere – whether consulting in a clinic, delivering telehealth, working in aged care facilities, or in a remote community.
GPRA President Dr Chris Dickie said patients are increasingly wanting to access their care from GPs and RGs via a variety of pathways – including digital platforms.
“The future is here, and the use of digital, safe and accessible platforms is just another way a doctor can keep in touch with their patient and vice versa, for the benefit of their health. While not replacing face-to-face care, the safe use of digital technologies is now a critical tool in the doctor’s service model. MediRecords recognises the unique needs of GPRA members as they embark on their professional journey.”
Dr Chris Dickie, GPRA President
With MediRecords, GP and RG registrars and early-career doctors can gain familiarity with secure, cloud-based systems that support flexible models of care. As they progress in their careers and transition into roles with greater autonomy, they’ll have the capability to build their practices using digital tools that enhance the way they deliver patient care.
As a fully cloud-based platform, MediRecords eliminates the need for on-site servers, offering a scalable, mobile solution that supports today’s increasingly flexible models of healthcare delivery.
Its API connectivity also allows doctors to innovate and integrate with other digital health tools, creating opportunities to build dynamic, patient-centred businesses.
MediRecords CEO Matthew Galetto welcomed the partnership, noting the alignment between the two organisations.
“MediRecords has a growing client base of early career, entrepreneurial doctors who want flexibility in their careers. Our platform gives GPRA members the freedom to work how and where they want, while leveraging our API connectivity to build truly exciting new healthcare businesses. It’s a great fit, and we look forward to supporting GPRA members as they shape the future of general practice.”
Matthew Galetto, MediRecords Founder and CEO
The partnership underscores a shared commitment to empowering the next generation of GPs with tools that meet modern healthcare demands, enabling mobility, connectivity, and innovation, while upholding standards of healthcare and quality general practice.
Partnering for better care: MediRecords joins forces with Doctors in Aged Care
October 28, 2025
MediRecords is proud to announce a new partnership with the Doctors in Aged Care (DiAC) community group – a fast-growing network of over 2,800 GPs and healthcare professionals dedicated to delivering care in residential aged care facilities (RACFs) and home settings.
This collaboration reflects a broader trend: more doctors are choosing cloud-based, mobile-first solutions to power their practices. With 57% of DiAC members identifying as women and nearly half aged between 35–44, the group represents a new generation of tech-savvy, entrepreneurial clinicians.
To support this shift, MediRecords is offering discounted licences to DiAC members, helping them streamline operations, integrate seamlessly with other platforms via our powerful APIs, and deliver care wherever it’s needed.
We’re excited to support DiAC members as they redefine what modern healthcare looks like, and where it happens.
MediRecords launches Engage Patient Portal to put patients at the centre of their care
October 8, 2025
Media Release
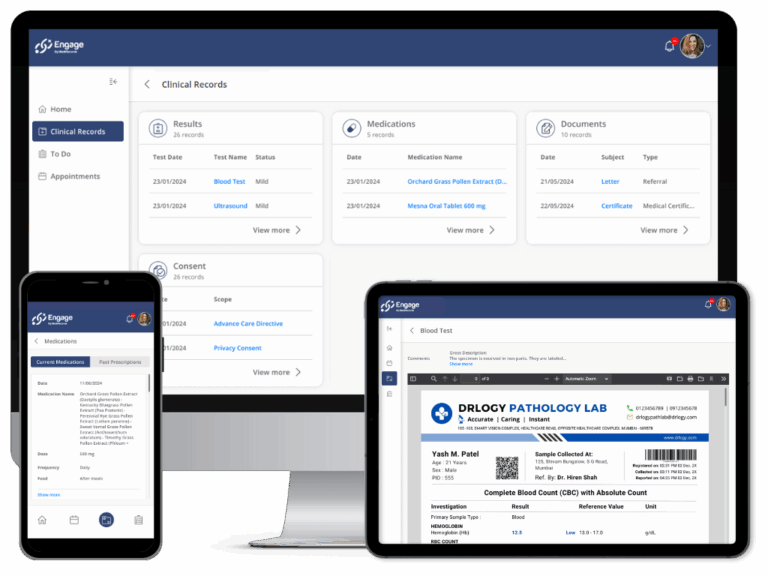
MediRecords has today announced the public launch of Engage, its new patient portal designed to improve communication, safety, and convenience in healthcare.
The Engage portal allows patients to:
Book appointments online
Securely store payment details
View their current medication list
Access and share results, correspondence, and education materials
Receive and complete tasks assigned by their healthcare team
Manage digital consent workflows.
By giving patients secure access to their records and enabling direct communication with their healthcare providers, Engage enhances safety and empowers people to take an active role in their care.
MediRecords CEO Matthew Galetto said the launch of Engage marks an important milestone in MediRecords’ mission to connect patients and clinicians on a single, cloud-based platform.
“Engage is the next step in our mission to connect patients and clinicians,” Mr Galetto said. “Building on the success of our existing patient portal, used by more than 150,000 patients, Engage delivers a more interactive, intuitive and fully white labelled experience. “It gives patients greater access to their health information and more control over how they manage their care, while giving practices the tools to streamline workflows, cut down on phone calls and improve patient safety. As we phase out our current mobile app and online booking tools in 2026, Engage represents the next generation of patient engagement, providing a single, seamless platform designed for the future of connected care.”
Engage integrates with MediRecords’ cloud-based clinical and practice management platform, allowing practices to streamline workflows while giving patients greater visibility of their health information.
The launch of Engage underscores MediRecords’ commitment to building a connected healthcare system that delivers better outcomes for patients while reducing the administrative burden on practices.
Is cloud technology the new necessity for innovation and productivity
in digital health?
September 23, 2025
Matthew Galetto - Founder and CEO MediRecords
Ask anyone working in digital health today, particularly those investing or looking for solutions to support new models of care, and they’ll tell you: all innovation is happening in the cloud. From startups launching AI diagnostic tools, coding agents, and voice assistants for booking and admin, to government projects aimed at connecting national health systems, everything modern is being built on cloud infrastructure.
Cloud is no longer a technology trend. It is the new normal.
At MediRecords, we see this shift as driven by more than convenience or cost-cutting. It is structural, it is inevitable, and it is being driven by real demand and expectations from service providers, clinicians, and most importantly, patients. In 2025, cloud-based technology has become the clearest signal of innovation in healthcare and the most practical way to achieve the productivity gains the system so urgently needs.
Whether you are a startup, a health service, or a government agency, cloud is no longer a nice-to-have. It is the bare minimum, and every new dollar of investment is chasing it.
Why cloud matters in digital health
The cloud is not just another way to host software. It is a different way to build, deliver, and keep improving it. Here’s why cloud-native solutions are leading the way:
Real interoperability: National health infrastructure is API-based, and that is where the future is heading. My Health Record, IHI, Provider Connect Australia, and the Service Locator are all part of an API ecosystem. Cloud-native systems are built to plug into these environments seamlessly, supporting information sharing at the point of care with the reliability and resilience of cloud hosting.
AI enablement: From clinical decision support to smart assistants and summarisation tools, AI runs best where it was designed to, on the cloud. Cloud makes AI scalable, secure, and accessible without the need for costly hardware. At the Medical Software Industry Association (MSIA) forum in July, AI was called out as both an opportunity and a risk. AI scribes, triage tools and predictive analytics are recognised as critical enablers of safety and efficiency, but there are also new cyber threats, with attackers using generative tools to launch sophisticated campaigns. Cloud platforms offer the enterprise-grade security, zero-trust frameworks and rapid patching that healthcare now requires.
Data-driven care: Cloud platforms unlock live analytics and reporting that go far beyond static PDFs or siloed spreadsheets. Think population health insights, service delivery metrics, and predictive alerts, available in real time.
Lower overheads: No servers to manage and no on-site maintenance. Cloud reduces the total cost of ownership while accelerating change. Less drag, more delivery.
Always up to date: Continuous upgrades mean your platform improves every few weeks, not every few years. That is the speed clinicians and patients expect today.
Productivity through scale and innovation: Cloud is not just about what is possible today, it is about what becomes possible tomorrow. From smarter workflows and automation to seamless integrations and flexible deployment models, cloud platforms open new ways of working. Providers can scale efficiently, deploy services faster, and deliver care in ways that traditional systems cannot support.
Cloud as the productivity engine
The recent MSIA conference sharpened this focus. Digital health reform is no longer about modernisation for its own sake; it is about driving system-wide productivity. Rising demand, workforce shortages and growing administrative burden mean the health system must deliver more with less.
Cloud-native platforms, built on FHIR standards and national interoperability, enable real-time data sharing, automation and AI in ways that reduce duplication, shorten wait times, and free up clinicians for patient care.
Seen this way, cloud is more than a proxy for innovation. It is the engine of productivity. In health, innovation and productivity are inseparable. Innovation that does not deliver productivity will not scale, and productivity gains without innovation will stall.
Government signals: Cloud as a strategic pillar
The federal government’s Sharing by Default Act 2025 is a milestone, requiring pathology and diagnostic imaging results to flow automatically into My Health Record. The upcoming National Digital Medicines Strategy (2025–2030) will go further, embedding interoperable, cloud-enabled medicines management into the foundations of the system.
Policy language now makes it clear: “information sharing by default, near real time, at the point of care” is the goal. That is only achievable with cloud-native systems that speak fluent API.
Procurement patterns are already shifting. It is increasingly difficult to win a government contract or even make it to tender without being cloud-enabled.
Clinicians are also driving this change. Next-generation doctors are digital natives. They expect intuitive, mobile-responsive, fast-evolving tools that feel more like Spotify or Canva than clunky desktop software. Patients expect the same: digital front doors, secure portals to access personal information, cost transparency, and notifications that help them manage their care.
Investment dollars also tell the story. Every new venture-backed digital health company in Australia is building for the cloud. There is simply no appetite to fund new on-premise apps.
Finally, security is no longer a barrier to cloud, it is a benefit. Cloud platforms provide enterprise-grade security, encrypted communications, and high availability that far exceed what most local deployments can offer. In today’s environment, cloud has become the safer, more resilient choice.
Evidence that digital maturity and connected systems delivers results
The evidence for digital transformation in Australia is compelling.
Queensland’s transition to integrated digital hospitals achieved a 40% reduction in medication incidents and a 70% reduction in prescribing errors.
Digital-first cardiac rehabilitation programs have demonstrated up to 71% reductions in readmission bed days, proving that connected care can improve outcomes and reduce costs.
Studies of digital maturity in Queensland health services show that higher-maturity, interoperable systems are associated with better patient experience, improved staff satisfaction, and perceptions of safer care.
Cloud as the path to digital maturity
These improvements arise from digital maturity, not hosting models alone. But cloud is increasingly the only realistic way to achieve and sustain that maturity at scale. Recent Australian examples demonstrate the benefits. NSW Health’s migration of clinical applications to AWS Cloud improved application performance, halved the time to deploy new environments, and freed clinicians from manual IT work. A trans-Tasman review of 66 cloud-enabled healthcare use cases found consistent gains in productivity, patient access, and system equity. And in community pharmacy, electronic prescribing and digital medication records, often delivered via cloud platforms, have streamlined workflows and improved medication safety.
Cloud does not just enable new technology; it provides the structural resilience, interoperability, and scalability that allow digital systems to deliver measurable improvements in outcomes and efficiency.
MediRecords: A case study in cloud-driven innovation
MediRecords was built in the cloud from day one, not retrofitted or migrated. That foundation lets us partner with the most forward-thinking health programs, providers, and digital vendors across the country.
We are already helping modern care models take shape:
AI partners are integrating with our APIs to provide summarisation, smart triage, and workflow automation.
Analytics through our soon-to-be-released Clarity module, giving providers real-time insights into service usage, clinician performance, and patient outcomes.
We connect natively with Australia’s API-based government digital infrastructure, ensuring our customers can operate seamlessly across national systems. Our containerised implementation of OntoServer (CSIRO’s terminology server) provides scalable clinical decision support and structured interoperability as a managed service.
Just as importantly, our open APIs empower healthcare organisations to shape their own digital future by connecting enterprise systems, building digital front doors for patients, and innovating beyond the clinic walls.
Conclusion: The cloud test
If you are evaluating a new digital health solution, whether it’s practice management, patient engagement, analytics or anything related, ask this first: is it cloud-native?
If not, it is already out of step with:
Where government policy is going
Where clinicians and patients expect to be
Where investment dollars are flowing
In 2025, cloud is not just infrastructure. It is the benchmark for innovation and productivity in digital health.
In healthcare, innovation that does not deliver productivity is unsustainable. Productivity gains without innovation pathways, quickly erode. Cloud is where the two converge, and where the future of healthcare is being built.
References
Queensland Health. Digital Hospital Benefits Realisation Report. Cited in MSIA, 2021.
Neubeck L, et al. Digital cardiac rehabilitation: systematic review and meta-analysis.Eur J Prev Cardiol. 2020.
Woodruffe S, et al. Effects of a digitally enabled cardiac rehabilitation intervention on risk factors, recurrent hospitalization and mortality: a randomized controlled trial.European Heart Journal – Digital Health. 2025
Adler-Milstein J, et al. Evaluating Digital Health Capability at Scale Using the Digital Health Indicator.Appl Clin Inform. 2021.
Thiru K, et al. Perceived Impact of Digital Health Maturity on Patient and Staff Experience in Queensland.Int J Med Inform. 2023.
eHealth NSW. Case Study: Clinical Applications Migrated to AWS Cloud. 2022.
AWS Institute. Benefits of Cloud-Enabled Healthcare in Australia & New Zealand. 2022.
Hussain R, et al. Electronic health records and e-prescribing in Australian community pharmacies.Int J Med Inform. 2024.