Tim Pegler - MediRecords Senior Business Development Manager


Australia has a unique set of problems to overcome, said David Rowlands, a member of the Roster of Digital Health Experts at the World Health Organization (WHO).
He told the October Wild Health Summit: “What we are seeing are symptoms of a fundamental failing of our health system.”
“Our health system was designed 50 years ago for problems of 50 years ago. (It) was not designed to deliver integrated, value-based care. It was designed to deliver episodic care.”
Episodic care is provided to patients who need treatment for an “episode” of care with a foreseeable “endpoint”. Examples include cases treated in hospital Emergency Departments.
The focus in Australia’s health care system, Mr Rowlands said, is on outputs, not outcomes.
Value-based care uses a model where providers, including hospitals and physicians, are paid based on patient health outcomes. Under value-based care agreements, practitioners are rewarded for helping patients improve their health, reduce the effects and incidence of chronic disease, and live healthier lives.
The “value” in value-based healthcare is paid after measuring health outcomes against the cost of delivering them.
In contrast, episodic care is paid on an activity-based or fee-for-service model measuring the amount of healthcare services delivered.
Mr Rowlands said tinkering with the system will fail. “After 50 years, it’s time for a review.” He said the Australian system needed independent, external experts to determine the way forward. He cited Lumos, a new partnership between the NSW PHNs and the NSW Ministry of Health, as an example of doing things differently.
Lumos generates insights into patients’ journeys across the health system and shares de-identified data from general practices with other health services to provide a comprehensive view of patient pathways.

Elisabeth Koff, the managing director at Telstra Health and immediate past secretary at NSW Health, said she had helped negotiate health agreements and most came down to money rather than a strategic approach to healthcare.
She said reform agreements focusing on outcomes had been negotiated but, “then we forget about them, and they sit on the shelf”.
While there had been progress in New South Wales around collaborative communities, Ms Koff said change would be slow as governments are focused on the short term and, “health care reform is hard… no pain, no gain”.
Tracey Johnson, the CEO and company secretary at Inala Primary Care, said Australia’s health system is run by “mini-empires”, each seeking individual advancement.
“We don’t have a healthcare system,” she said. “We have a profile-for-profit system.”
Inala reinvests any practice profits into patient care, but it was becoming difficult to provide affordable care when reliant on a $39 bulk-billing item.
Ms Johnson said General Practice should be considered a specialist form of medical care, given the knowledge and training required. This could provide access to a wider range of Medicare-funded billing items.
Ms Johnson pointed to the role GPs play in taking pressure off overcrowded hospitals. “Data shows where patients visit their GPs more, there were fewer hospital admissions… Comprehensive care works.”
MediRecords is used by general practitioners, specialists, multidisciplinary clinics and hospitals across Australia. The MediRecords electronic health records platform features embedded SNOMED CT-AU coding and is designed for interoperability using FHIR and APIs. MediRecords is currently developing additional functionality to support team case management and value-based care.
If you are interested in learning more about MediRecords’ functionality to support team case management and value-based care, book a demo below.

A recurrent theme was that telehealth has been normalised during the pandemic and is now an everyday tool for doctors and specialists. But while digital and virtual care technology is widely used, too many systems still don’t share information and healthcare professionals are fed up with having to use multiple, disconnected products.
Here are some snapshots from the festival:
Australian Digital Health Agency CEO Amanda Cattermole said the agency remains committed to a connected healthcare system through which data passes, “seamlessly, safely and securely”. Ms Cattermole said a new National Digital Health Strategy is imminent and that the ADHA has three key roles:
ADHA projects under way also include:

My Emergency Doctor founder and Medical Director Justin Bowra explained how virtual ED doctors help improve patient flow and reduce clinical risks at hospitals and urgent care centres. Dr Bowra said MED clinicians conduct case conferences via video calls, including reviewing the status of patients waiting in ambulances. The case conferences enable patient flow decisions that reduce ED wait times, such as advising that patients can go direct to theatre. The service also provides clinical decision support and mentoring to on-site doctors and an auditable recording of all interactions.
Caligo Health Managing Director Dr Amandeep Hansra said the COVID-19 pandemic had catapulted digital health innovation forward by at least a decade, creating created consumers who are actively engaged in their care and demand access to and control of personal data. The pandemic had also created a mountain of data — 30% of global data comes from health — that could be the foundation for scalable analytics and AI-driven businesses.
e-Health Queensland Health Deputy Director General Damian Green walked festival goers through the Sunshine State’s digital strategy, emphasising the importance of human-centered design and delivering equitable healthcare access for First Nations peoples and diverse communities. Mr Green said clinicians were required to work with too many products and ‘system sustainability’ would necessitate fewer systems with the requisite data for better decision making. He said safety was at the heart of all digital investment decisions and told vendors, “if you can show you are going to improve outcomes, then talk to us.”
Victorian Department of Health Chief Digital Officer Neville Board placed patient safety as the destination for the Garden State’s digital health roadmap. Mr Board said reducing risks to patients caused by paper-based processes was a major priority and showed how e-prescribing significantly reduces risks of medication errors. Victoria has also committed to a Health Information Exchange that enables interchange of information between all hospitals.
Neville Board placed patient safety as the destination for the Garden State’s digital health roadmap. Mr Board said reducing risks to patients caused by paper-based processes was a major priority and showed how e-prescribing significantly reduces risks of medication errors. Victoria has also committed to a Health Information Exchange that enables interchange of information between all hospitals.
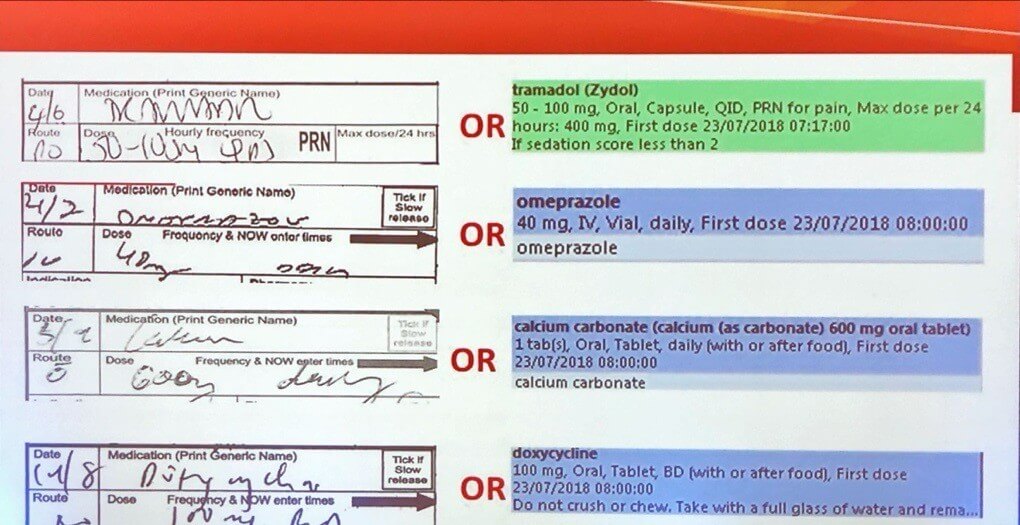
Victorian Chief Digital Officer Neville Board highlights the risks of handwritten medication notes.
Alcidion CEO Kate Quirke said procurement processes in Australia were a deterrent to innovation and that many Proof of Concept projects did not proceed to implementation because contractual requirements were too onerous.
Former Deputy Chief Medical Officer Dr Nick Coatsworth said healthcare start-ups need to be thoroughbreds capable of going the distance, rather than flashy unicorns. And the secret to designing an enduring product? Make sure you’re solving problems for patients and their families.
Dr Emma Rees, Founder and CEO of women’s healthcare platform Femma, said health care should not cease when a patient leaves the room and be suspended until a follow-up appointment. Dr Rees said “the future of healthcare is a hybrid model” where patients have clinically curated, individual management plans and on-demand access to education materials and nutritional, exercise, mindfulness and yoga programs.
Image courtesy of ResApp
Australian start-up ResApp has developed a digital diagnostic app for respiratory illnesses, available on mobile devices. The ResApp tool listens to a patient cough five times and then sends a report direct to a GP. ResApp CEO Dr Tony Keating said trials in India and the US had shown a high level of accuracy in diagnosing COVID-19. Using the app for initial diagnosis could make up to 80% of RAT and PCR testing unnecessary, bringing immediate benefits for patients, cost savings for governments and environmental benefits.
The Global Healthcare Lead for Zoom, Ron Emerson, said research by a leading US healthcare provider had shown that 70 per cent of patients attending at urgent care facilities could be safely seen by a virtual health care clinician, helping to relieve pressures on overcrowded hospitals. Zoom is now being used by prestigious US healthcare organisations, including the Mayo Clinic, Johns Hopkins and New York Presbyterian hospitals.


Throughout July we ran a survey for users of Medical Practice Management Software, like MediRecords. The aim was to listen to, and learn from, both our own users and those who use alternatives.
In this article we have summarised some of the more interesting insights around:
If any of this sounds interesting, then please read on! But before we get into it, we would like to say a big thank you to all who took part in the survey.
As with all survey data, the stats can often be interpreted in many ways. If you have any insights or explanation for what we found in the survey, we would love to hear from you via [email protected].
Our survey was delivered to GP clinics via fax, email and through The Medical Republics e-newsletter. Whilst the survey was open to clinicians, practice managers, nurses and business owners, most respondents primarily identified as clinicians.
We ran our survey throughout July, which ended up being an interesting time. The initial explosion of conversations around Telehealth had begun to quieten down (more on this later), whilst Victorians began seeing lockdown restrictions gradually being enforced as they experienced their ‘second wave’.
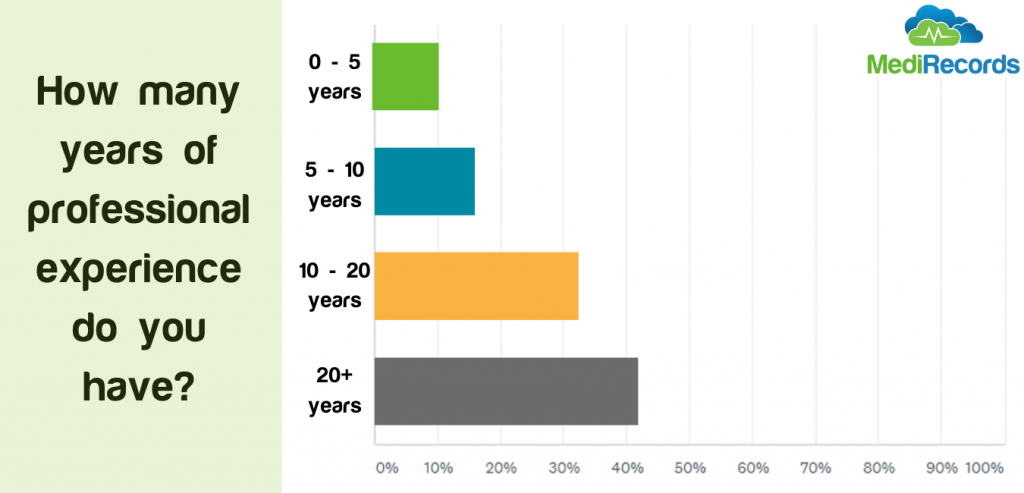
One noticeable skew was that the audience had a significant amount of professional experience, with over 40% having over 20 years in General Practice, which is worth bearing in mind as you read this article:
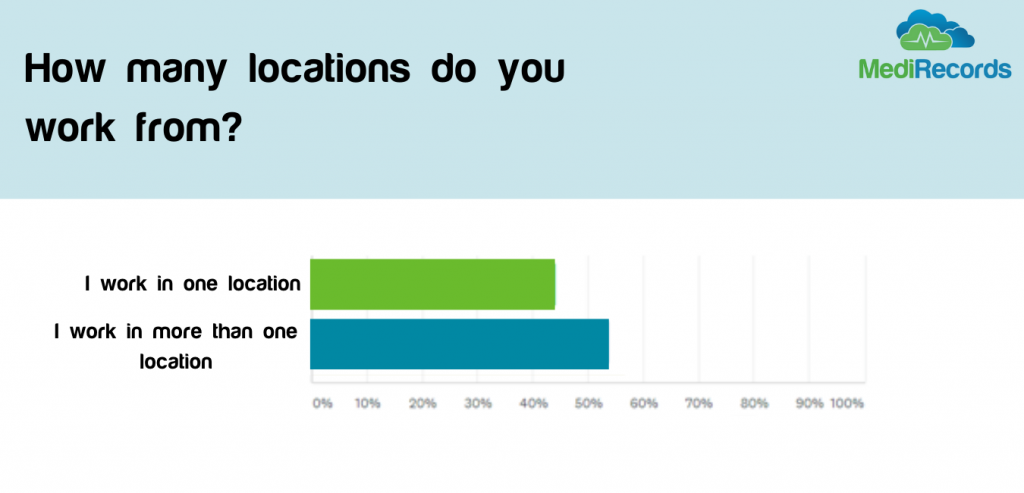
We were keen to understand how GPs tend to work, as this allows us to better understand how MediRecords can be as useful to clinicians as possible.
We found GP’s were split fairly evenly between those who work in one location, and those who work across multiple locations. What is not clear if this means they work across multiple practices, or often from home, something which could be influenced by the current pandemic.
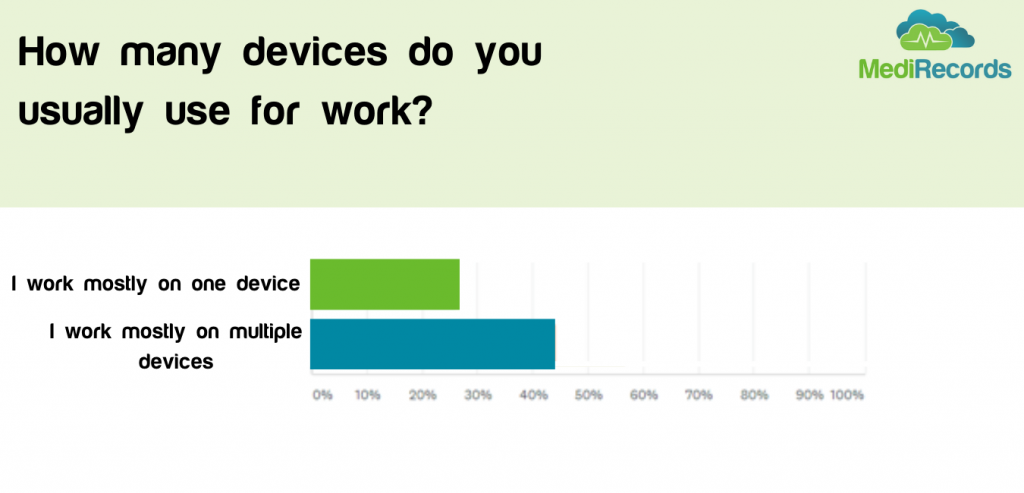
Far more clinicians work on multiple devices rather than one, which us unsurprising given our consumer habits across phones, tablets and computers. It is particularly interesting for practice management software however, as ease of working across devices and locations is very difficult on server-based solutions such as Best Practice and Medical Director, compared with cloud solutions like MediRecords.
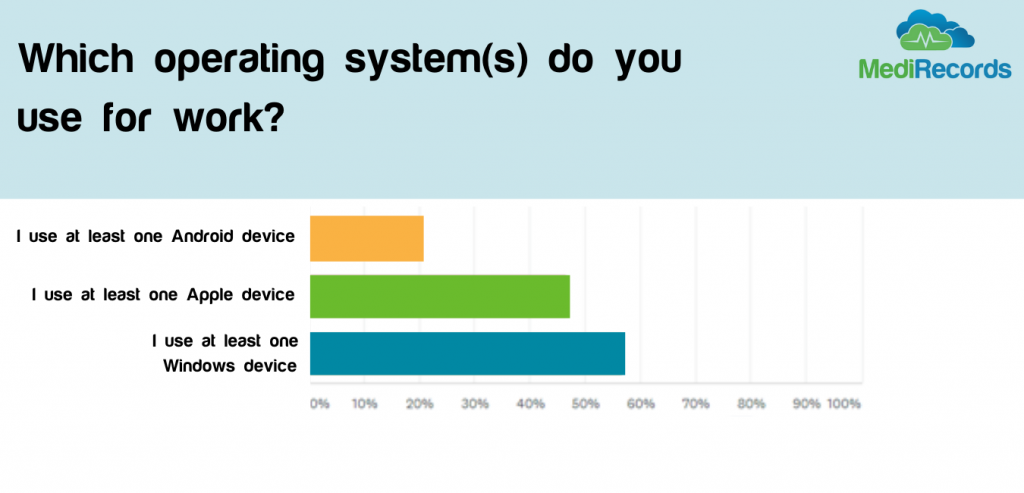
It was interesting to see that almost as many people use Apple products as do Windows, again something that could make browser-based software more appealing to ensure consistency of experience and usability for GPs on whichever device they use.
We asked our GP respondents a lot of questions about their preferences are for practice management software. This information is best summarized in the two questions:
Surprisingly, the same sort of answer was most popular for both questions – Usability!
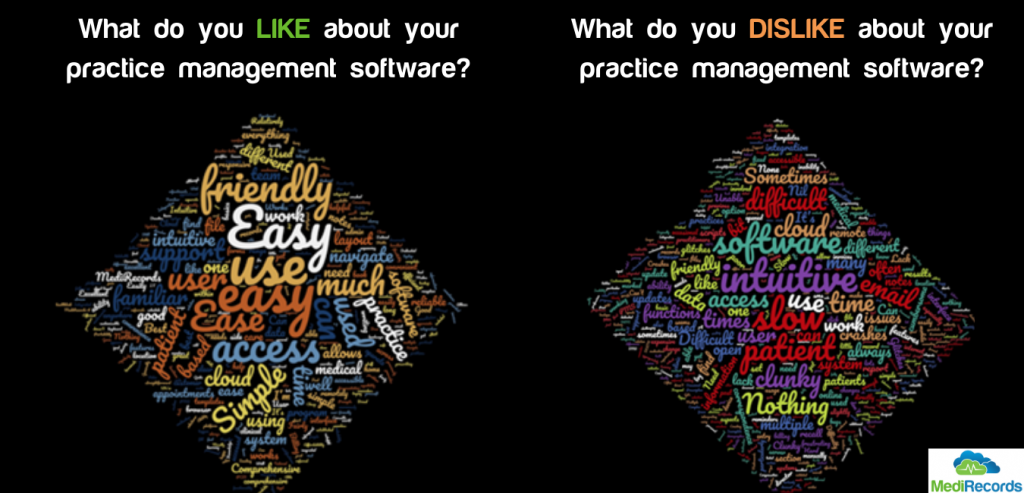
It can be easy to get lost in specifications and functionality lists when choosing Practice Management Software, but what this shows us all is that, fundamentally, it means little if the platform is not easy for clinicians to use. We suspect this will also be what drives most day to day frustrations users have with their current software.
(By the way, we think this is great news given the positive feedback we have had on MediRecords from our users. If you are struggling with usability there is a solution!)
We then asked if clinicians were planning on reviewing or upgrading their software over the next five years. Only 40% of respondents said they would consider doing so.
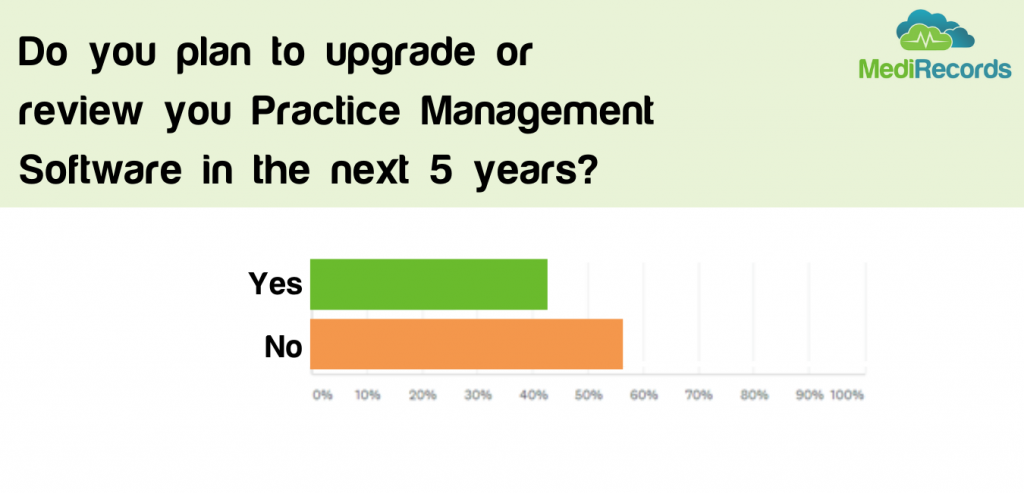 Many in the healthcare tech space may find this disappointing, but we believe it shows us the wider trend of reluctance to adopt and change with new technologies. Whilst many may be heralding a silver lining of COVID to be increased adoption of technology, the results suggest this mindset change will not happen overnight – even if pushed by a major event such as COVID.
Many in the healthcare tech space may find this disappointing, but we believe it shows us the wider trend of reluctance to adopt and change with new technologies. Whilst many may be heralding a silver lining of COVID to be increased adoption of technology, the results suggest this mindset change will not happen overnight – even if pushed by a major event such as COVID.
We asked respondents to rank features in terms of the importance to them when choosing practice management software. Whilst we won’t be sharing the full results of this (hopefully you can understand, we want to keep some knowledge to ourselves!) what was surprising was that Telehealth was the second least important feature to the GPs we asked.
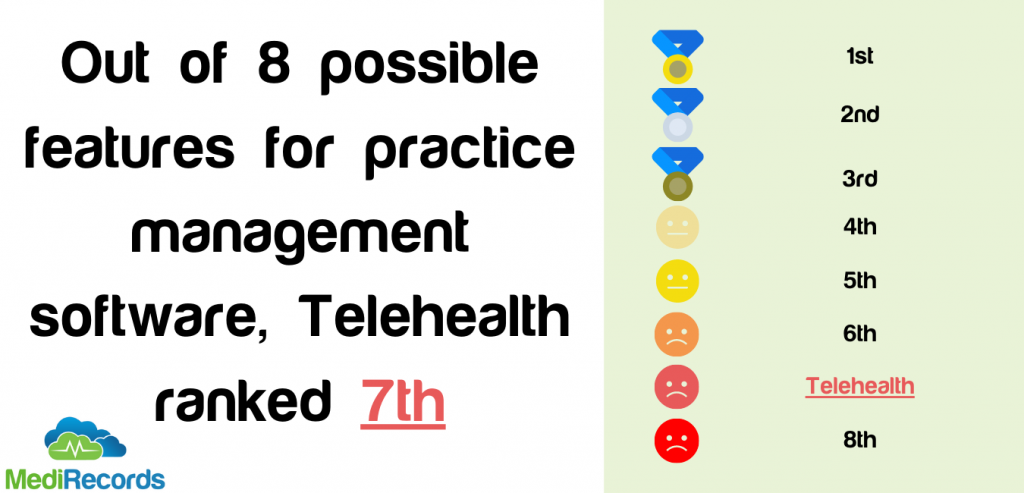
The timing of the survey may have had something to do with this. Whilst in the earlier days of the pandemic many GPs were trying to figure out how to incorporate Telehealth into their daily workflow, by July Telehealth MBS items had been live for over a month, with GPs finding that using the telephone was an easier, more familiar solution in the short term.
Again, this may reflect the reluctance of many to adopt new technologies, even if these technologies lead to better experiences for patients. We can see the benefits of telehealth via remote monitoring via projects such as Spritely’s recent trial in retirement villages in Christchurch, but clearly there is more work to be done to help clinicians see if there is a benefit for them.
Finally, we asked what GPs wished their PMS could do that it does not already.

The results here were less clear, with 27% of people wanted a feature specific to their practice’s requirements, and a further 20% wanting an integration with a specific other service.
This shows how personal and bespoke the needs of many practices are, and how software such as MediRecords must not only be flexible for different workflows, but also responsive to users when they need new feature.
Again, usability came up, this time as something that respondents wish their PMS offered. Given the large share of the market enjoyed by traditional solutions such as Medical Director and Best Practice, perhaps this reflects the need for clinicians to look at some of the newer, easier to use options that are out there.
Personally, we think MediRecords fits the bill perfectly! If you would like to find out more you can contact [email protected], book a demo, or enjoy a 30 day free trial now.
Andrew Dyson is our Digital Marketing Lead here at MediRecords, and managed this latest survey. Prior to joining MediRecords he has worked on marketing projects, including in depth market research, for some of the largest employers in the UK.

It may not make you a better GP, but experiencing grief is part and parcel of long-term care, writes Dr Bastian Seidel
Continue reading